Healthy lifestyles in childhood cancer survivors in South Korea: a comparison between reports from children and their parents
Article information

Abstract
Purpose
This study investigated childhood cancer survivors' behavior related to a healthy lifestyle during their survival period by comparing reports between childhood cancer survivors and their parents.
Methods
In this comparative descriptive study, a survey was conducted with a 33-item questionnaire and one open-ended question about areas for improvement. The participants comprised 69 childhood cancer survivors and 69 of their parents, for a total of 138.
Results
The total mean healthy lifestyle score, on a 4-point Likert scale, reported by childhood cancer survivors was 2.97, while that reported by their parents was 3.03. No significant differences in children's healthy lifestyles were found between childhood cancer survivors' and their parents' reports (t=0.86, p=.390). For the open-ended question, the main keywords based on the results of degree and eigenvector centrality were "exercise", "unbalanced diet", and "food". These keywords were present in both the children's and parents' responses.
Conclusion
Obtaining information on childhood cancer survivors' healthy lifestyles based on reports from themselves and their parents provides meaningful insights into the improvement of health care management. The results of this study may be used to develop and plan healthy lifestyle standards to meet childhood cancer survivors' needs.
INTRODUCTION
In recent years, the survival rate of childhood cancer patients has increased dramatically, owing to innovative medical technology and advances in treatment. Consequently, the population of childhood cancer survivors (CCS) is rapidly growing worldwide [1-3]. In North America, the overall 5-year survival rate of CCS is over 80%[4,5]. Similarly, according to a Korea Disease Control and Prevention Agency report, the average 5-year survival rate of childhood cancer in Korea has increased to 80%[6].
However, because of therapy-related complications, up to 70% of CCS suffer from at least one chronic health problem after completing treatment [1]. CCS are generally considered a distinct and vulnerable group, as children who survive cancer continue to be at risk of developing health issues that persist years after completing cancer treatment [3,7-9]. Multiple health conditions result in a high cumulative chronic disease burden in CCS [1]. Therefore, specialized screening and lifestyle management are required for the early detection and prevention of late effects. A healthy lifestyle (HLS) may lead to better clinical outcomes in CCS [9]. The impact of physical and psychosocial effects is often linked to health-related quality of life. From this point of view and considering their scores in HLS measurements, CCS have poorer than average experiences of childhood [1]. Understanding these aspects may lead to a successful transition from the completion of cancer treatment to optimal long-term surveillance. In addition, HLS factors may not only help diminish the risk of chronic health conditions but also promote the health of CCS.
Children between 6 and 12 years old are in a period of concrete operational cognitive development, developing the sense of industry, their own perspectives, and acquiring new technology in daily life [10,11]. In addition, they illustrate the virtues of active work, a practical approach, and the developmental progression of illness knowledge. Thus, they may be able to take healthy actions and modify behaviors, such as unhealthy lifestyles.
The importance of the daily functioning of CCS has emerged as a research focus in recent years [11]. However, related information is only available to a limited extent, although CCS need such information to maintain and promote an HLS. In this regard, a daily HLS is salient to a CCS's life. Long-lasting interruptions in daily life may have lifelong psychosocial and socioeconomic consequences [12]. Hayek et al. [13] identified that CCS showed a higher prevalence of frailty than their siblings or peers. They suggested that promoting an HLS is needed to decrease the prevalence of frailty and preserve function in this at-risk population. Building connections between children's daily function and HLS can impact their overall quality of life, but existing research on survivorship services is limited [14]. Providing care for these patients requires identifying and recognizing their HLS. Moreover, children's HLS is strongly influenced by their parents' nurturing style and the surrounding environment [11]. Therefore, obtaining information on the HLS of CCS as reported by the children themselves and their parents may be the first step toward planning and implementing nursing interventions for maintaining positive health outcomes.
This study aimed to characterize the everyday behavior of CCS in terms of their HLS during their survival period. Thus, we took the following steps: 1) obtaining information on the HLS of CCS as reported by CCS themselves; 2) obtaining information on the HLS of CCS as observed by their parents; 3) comparing children's and parents' reports of the HLS of CCS; and 4) identifying aspects of HLS needing improvement as reported by CCS and their parents.
METHODS
Ethics statement: This study was approved by the Institutional Review Board (IRB) of Sahmyook University (No. 2021082HR). Informed consent was obtained from all participants.
1. Study Design
This was a comparative descriptive study conducted to identify differences in children's reported HLS as described by CCS and their parents.
2. Participants
A survey was conducted among CCS and their parents who were registered as members of the Korea Pediatric Cancer Foundation and agreed to participate in this study. The eligible CCS participants were those who were 1) of school age (6-12 years old), 2) diagnosed with cancer and had completed treatment, 3) able to read and understand questionnaire items, and 4) willing to participate. The parents of all CCS were required to provide consent. In addition, parents of CCS who agreed to participate in this study were also surveyed. The exclusion criteria were severe psychiatric or cognitive conditions hindering participation in a questionnaire survey.
The calculation of the appropriate sample size was based on a previous cross-sectional study [15] that identified the physical, psychological, and social needs of adolescents and young adults. Using G*Power version 3.1.9 [16] with the independent t-test as the main analysis method, the power (1-β) was set at .80, the significance level (α) at .05, and the effect size (d) at .50, and the obtained total sample size was 128 (64 per group). Considering a dropout rate of 10%-20%, 75 participants were initially recruited for each group. The final data analysis in this study included a total of 138 participants: 69 in the CCS group and 69 in the parent group.
3. Procedures
Prior to conducting the research, institutional review board approval was obtained from the research committee of Sahmyook University (No. 2021082HR). The Korea Pediatric Cancer Foundation was asked for cooperation after the purpose of the study was explained. Through the Korea Pediatric Cancer Foundation, an announcement was made regarding the purpose of this study, the study participants (school-age CCS and their parents), the survey content and method, and gifts provided after the survey. With participants' permission, their phone numbers were collected.
After a trained researcher called the participants individually to explain the purpose of the study and the survey method, a Google Forms questionnaire containing written consent was sent to the children and parents, respectively. The online survey was conducted from August 25 to September 30, 2021, and it took 10 to 15 minutes to complete. An online gift card was sent to the subjects who completed the questionnaire.
4. Measures
The conceptual framework (Figure 1) of this study drew upon the Adolescent Lifestyle Profile-Revised 2 (ALP-R2) tool developed by Gaete et al. [17] to analyze the HLS of CCS. The ALP-R2 tool consists of seven sub-dimensions with a total of 44 items, including health responsibility (7 items), physical activity (6 items), nutrition (7 items), positive life perspective (6 items), interpersonal relations (6 items), stress management (6 items), and spiritual health (6 items). The total scale reliability of the ALP-R2 was shown by a Cronbach's α of .87.
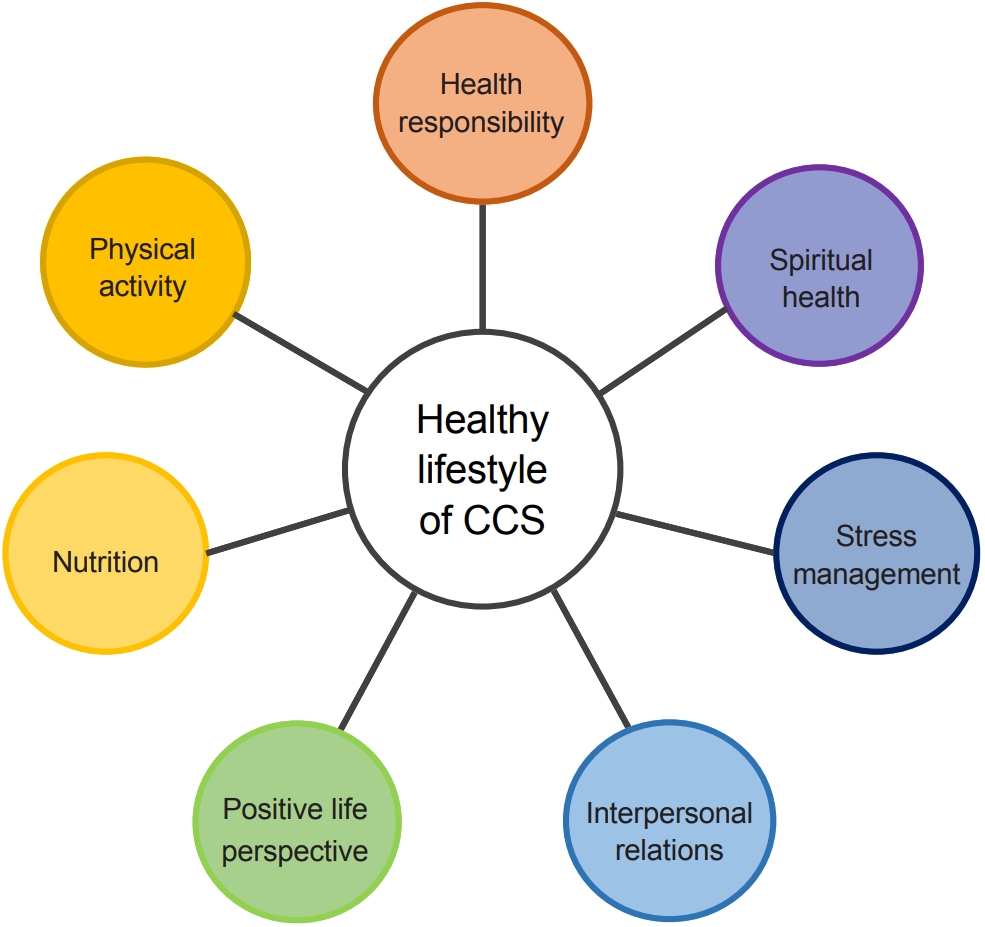
Conceptual framework. CCS, childhood cancer survivors.
In this study, the number of items was reduced to fit school-age developmental characteristics. Permission for using the tool was obtained from its developer. In addition, it was agreed that the content validity would be verified after reducing and modifying the items according to the characteristics of school-age children. The process of reducing and revising the tool items was as follows.
First, the items of the ALP-R2 tool were translated into Korean by a nurse who could speak English at a bilingual level. Second, after researchers reviewed the 44 translated items, 34 items were selected, and the words and context were modified to suit the comprehension level of school-age children. Third, the initial version of the translated and revised tool was tested for content validity on eight healthy elementary school students. Each item was rated from 1 (not at all appropriate) to 4 (very appropriate) on a 4-point Likert scale, and participants were asked to freely express their opinions on individual items. A content validity index of .74 was observed. The revised tool, reflecting the results of the primary content validity test, was subjected to a secondary content validity test by eight experts in nursing for children with cancer (four professors of nursing, one social worker at a pediatric cancer hospital, one pediatric oncologist, and two nurses at general hospitals). A content validity index of .82 was obtained. One of the four spiritual health items was deleted, based on the received opinions on content validity, resulting in a total of 33 items. The revised tool, reflecting the results of the secondary content validity test, was tested for tertiary content validity by two children with cancer and two parents. A content validity index of .86 was observed.
Fourth, after three rounds of content validity verification, the 33 revised items were reverse-translated by two bilingual middle school students and a nurse living in the United States. A total of four people (three nursing professors and one bilingual nurse) checked the agreement of the reverse-translated version with the original text. The consistency of the 33 items was 88%-100%.
After translation, content validity, and reverse-translation, the final confirmed tool contained 33 items including health responsibility (6 items), physical activity (4 items), nutrition (4 items), positive life perspective (5 items), interpersonal relations (6 items), stress management (5 items), and spiritual health (3 items). For parents' assessments of the HLS of CCS, the subject of the 33 items was changed from "I" to "my child."
In this study, the reliability of the 33 items identified in the data collected from CCS and their parents was shown by Cronbach's α values of .90 and .87, respectively. As general characteristics, CCS were asked to provide information on their gender and age. Table 1 shows the characteristics of CCS and their parents. One open-ended question was asked to both CCS and parents: "What am I (or is my child) not doing well in order to be healthy?".

Description of the Sample According to Demographic Variables (N=138)
5. Data Analysis
The demographic information and quantitative survey results were analyzed as descriptive statistics using SPSS for Windows version 26 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean and standard deviation, and categorical variables were presented as frequencies and percentages. The independent t-test was used to analyze differences in children's reported HLS between CCS and their parents.
The answers to the open-ended question regarding areas for improvement in HLS were analyzed using NetMiner version 4.0. The node filtering process was applied only to nouns as morphemes [18]. After importing an Excel file using the unstructured data function in NetMiner, 62 words from the CCS data and 96 words from the parental data were initially identified in the main node set. Two researchers reviewed word frequency to determine the cut-off criterion; as the data were concise, they decided to reflect upon and analyze them all. In this process, unnecessary words and those related to research methods were removed. Three representative types of dictionaries (a thesaurus, defined words, and an exception list) were developed. The main words ("health", "lifestyle", and "child") included in the research title were excluded. In developing the co-occurrence matrix for keywords, a one-mode network was generated from a two-mode network, using the recoded weight value of term frequency-inverse document frequency. An inner-product-proximity measure was adopted during the mode-conversion process. Link reduction was not performed due to the small quantity of data, and the degree centrality and eigenvector centrality were obtained for the main analysis.
Degree centrality measures the number of connections carried by a single node; a node with a higher degree centrality value and a higher number of connections within a network is a core keyword [19]. Eigenvector centrality overviews the entire network to discover the most influential keywords by counting their surrounding neighbors. The standardized value of centrality, which lies between 0 and 1, is used to determine the core keywords in the theme of a study [18,19].
RESULTS
1. Participants' Characteristics
1) Child-related characteristics
The child participants were 37 girls (53.6%) and 32 boys (46.4%). Their mean age was 9.5 (standard deviation [SD]= 2.0) years, and the average age at the time of cancer diagnosis was 4.6 (SD=2.9) years. The most common type of cancer was leukemia, which was present in 41 (59.4%) CSS. The treatments they received were chemotherapy for 50 (72.5%), hematopoietic stem cell transplantation for 28 (40.6%), surgery for 25 (36.2%), and radiotherapy for 16 (23.2%). Among the children, 54 (78.3%) had no recurrence, while 15 (21.7%) experienced recurrence. The health status perceived by the CCS was moderate in 29 (42.0%), healthy in 21 (30.4%), not healthy in 13 (18.9%), and very healthy in 6 (8.7%) (Table 1).
2) Parental characteristics
Most of the surveyed parents were mothers (65, 94.2%). The parents' age ranged from their 30s (43.5%) to 40s (56.5%). Most were college graduates (n=50, 72.5%), and almost all parents (66, 95.7%) were married. Forty-eight parents (69.6%) were from the middle class. Thirty-five (50.8%) had no religion, and 20 (29.0%) were Protestant (Table 1).
2. Childhood Cancer Survivors' Healthy Lifestyles Reported by Themselves and That Observed by Their Parents
The total mean HLS score in CCS was 2.97 (SD=0.39). The mean scores of the sub-dimensions were as follows: stress management, 3.30 (SD=0.55); interpersonal relations, 3.22 (SD=0.43); positive life perspective, 3.16 (SD=0.51); health responsibility, 2.87 (SD=0.41); nutrition, 2.84 (SD=0.50); physical activity, 2.77 (SD=0.68); and spiritual health, 2.25 (SD=1.05).
The total mean score of children's HLS reported by their parents was 3.03 (SD=0.31); The mean score among sub-dimensions were as follows: stress management, 3.34 (SD=0.39); positive life perspective, 3.22 (SD=0.39); interpersonal relations, 3.21 (SD=0.39); health responsibility, 2.99 (SD=0.39); physical activity, 2.84 (SD=0.69); nutrition, 2.82 (SD=0.52); and spiritual health, 2.36 (SD=1.01).
3. Differences in Children's Healthy Lifestyles between Childhood Cancer Survivors' and Parents' Reports
There was no significant difference between the HLS scores reported by the CCS themselves and the HLS scores reported by their parents (Table 2). Moreover, the seven sub-dimensions showed no statistically significant differences in reports between CCS and their parents.

Childhood Cancer Survivors' and Their Parents' Reports on Children's Healthy Lifestyles (N=136)
4. Areas for Improvement in Healthy Lifestyle-Related Behavior Reported by Childhood Cancer Survivors and Their Parents
The results of the degree and eigenvector centrality for the response to the open-ended question (What am I (or is my child) not doing well in order to be healthy?) are as follows (Table 3). Among the children's own responses, the main keywords belonging to the top 10 were "exercise", "unbalanced diet", "food", "cellphone", "instant", "temptation", "body", "meal", "snack", and "computer". Among parents' responses regarding their children's unhealthy practices, the main concepts belonging to the top 10 were "unbalanced diet", "exercise", "self-control", "food", "body", "vegetable", "environment", "cellphone", "needs", and "treatment".

The Degree and Eigenvector Centrality of Keywords Regarding the Open Question
DISCUSSION
The increasing survival rates of CCS, which exceed 80%[13,20], imply that HLS is a key concept for maintaining and promoting the health status of these children. In this study, the HLS reported by the CCS and their parents showed a moderate level, including sub-dimensions, except for "spiritual health".
Stress management had the highest HLS score among the seven sub-dimensions. Emotional stability may be linked to CCS' health during the period of survival. In the current study, although the HLS score of stress management placed it in the most desirable position among the seven sub-dimensions, some types of childhood cancer may enhance children's susceptibility to a number of psychosocial effects, such as loneliness, depression, and withdrawal from society [20]. Compared to other children, CCS are also prone to an increased risk of traumatic stress syndrome [20]. Although previous studies have shown that pediatric cancer survivors did not complain about psychological symptoms, during the transition from the acute to survivorship period, anxiety may continue to affect their physical well-being through a variety of mechanisms [21]. Barone et al. [22] reported that psychological distress and emotional symptoms were observed in 13% to 29% of adolescent survivors. The identification of stress management may aid CCS in choosing appropriate coping strategies in their present life.
Regarding interpersonal relations, CCS may be unable to maintain close relationships due to frequent treatments and limited contact caused by unexpected health problems. Social isolation is a significant challenge for CCS, impacting their everyday life even years after cancer was cured. Because of the long-lasting impacts of cancer on their peer relationships, they may distance themselves from their friends. Peer support plays an important role in decreasing stress and increasing adaptive coping in CCS [23]. Supportive relationships with parents and peers may serve to protect CCS from distress and help them have higher self-esteem [23].
The positive life perspective showed above-moderate levels in our study on HLS. Similarly, Andres-Jensen et al. [12] observed that cancer survivors generally viewed their health positively. By contrast, Bradford et al. [15] reported that adolescents and young adults had lower health-related quality of life than their healthy peers. Everes [24] explored the emotions of adolescents and young adults who experienced cancer, showing that they had both positive and negative life perspectives, possibly including fear, frustration, comfort, worry, belonging, trust, loneliness, acceptance, encouragement, connectedness, shame, guilt, pride, safety, and love. In this study, CCS seemed to consider and accept themselves as overall healthy, with their parents having a similar attitude. These findings imply that there are differences in positive life perspective between CCS and young adult cancer survivors. Therefore, CCS need help to adapt to their physical condition and have a positive view of their own health [12]. The three sub-dimensions (stress management, interpersonal relations, and positive life perspective) showing mean scores above 3 points had different aspects in comparison with adolescent and young adult cancer survivors, which may imply the relevance of these factors as developmental characteristics.
In the health responsibility sub-dimension, CCS scored higher than 2.5 points on the 4-point Likert scale. A survivor is defined as a person who is free of a life-threatening disease for at least 5 years [3]. According to a recent research report, the name "survivor" is regarded as a concept associated with overcoming adversity in those who have had cancer, and it is associated with a positive image [25]. It has also been reported that identifying as a cancer survivor can motivate children to actively cope with diseases by promoting awareness of the need for continuing medical management even after cancer treatment is completed [26]. In this study, the need for nursing intervention to help CCS take responsibility for their own health care was investigated by analyzing the degree of health responsibility among CCS.
The nutrition score was lower-ranked among the seven HLS sub-dimensions. Recent studies on the health-related quality of life of CCS published in Korea have only reported the results for physical, informational and healthcare system-related, psychosocial (related to school life), financial, and positive self-motivation needs, while few studies have investigated nutrition management [27]. In contrast, in international research on CCS, several systematic reviews or meta-analyses have reported the positive effects and importance of dietary interventions on the health-related quality of life of CCS [28]. In this study, the results for degree and eigenvector centrality showed a high demand for nutrition based on the main keywords (e.g., unbalanced diet, food, instant). This result may be related to CCS having more assistance from nurses for self-care.
Recent data indicate that more than 50% of CCS are at risk for exercise intolerance [13]. This study showed relatively low scores for the physical activity of CCS. In general, physical activities among children are likely to lead to other social activities and emotional enjoyment, thereby contributing to regular engagement [5]. Consistent with the results of this study, Australian CCS had a lower level of physical activity during survivorship than government recommendations and the general population [5]. Enhancing physiological capacity may not only improve the general health condition and wellness, but also emotional health, the ability to optimally participate in social roles, and the perception of quality of life among adult survivors of childhood cancer [13].
Spiritual health had the lowest score in this study. Spiritual well-being can provide CCS and their parents with positive coping strategies to find meaning and purpose in life during the survivorship period, and it may promote CCS' well-being beyond a cancer diagnosis into survivorship, since it has a protective role, reducing anxiety and depression [2,21]. A high level of life meaning/peace is more likely to generate better mental health and quality of life for CCS [21]. In Korean culture, there is a need for more in-depth explorations regarding the awareness of spiritual health among CCS and their parents.
CCS require much attention because they still have substantial unmet needs related to poorer quality of life that should be addressed. Both parents and nurses are encouraged to pay particular attention to four sub-dimensions (health responsibility, nutrition, physical activity, and spiritual health). Since the present study compared self-reported findings for the HLS of CCS with HLS as perceived by parents, the reliability of the self-reported results was ensured, as there were no significant differences in the mean values between the two groups in any of the seven sub-dimensions and total scores. Nurses are essential for CCS survivors and their families to ensure appropriate survivorship care and care coordination after the completion of cancer treatment [29]. This study has some limitations that should be noted. First, the participants in this study were recruited from a single center (Korea Pediatric Cancer Foundation); thus, this sample was not representative of the entire CCS population. Second, the results were derived from questionnaires filled out by children and their parents through self-reporting (subject to reporting and recall bias) independently in order to avoid mutual influence, instead of by having investigators observe their behaviors (performance). This study found no significant difference between children's and parents' responses regarding the HLS of children. However, further study would be necessary to determine whether significant differences exist in any factors that influence these responses. Finally, the revised 33-item tool that was modified to be suitable for CCS based on the original tool (ALP-R2) requires re-verification to confirm its reliability and validity with an expanded number of participants in future studies.
CONCLUSION
The findings of this study identified aspects (health responsibility, nutrition, physical activity, and spiritual health) that are particularly important for enhancing HLS in CCS. These results could provide a basis for further studies on specialized follow-up care and survivorship programs for the CCS population. Our study may not only prove useful for CCS and families for directing survivorship care, but also be helpful to cancer survivors in other developmental stages. Consequently, the findings of this study might help nurses become aware of the importance of HLS among CCS and their parents, and enable them to support CCS in implementing an HLS by acquiring knowledge about self-care for their own health.
Notes
Authors' contribution
Conceptualization: all authors; Data collection, Formal analysis: all authors; Writing-original draft, Writing-review and editing: all authors; Final approval of published version: all authors.
Conflict of interest
No existing or potential conflict of interest relevant to this article was reported.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (No. 2020R1A2C1100912).
Data availability
Please contact the corresponding author for data availability.
Acknowledgements
None.