INTRODUCTION
South Korea has recently entered the low birth rate era as women tend to delay marriage and pregnancy. However, with advances in medical science, the numbers of preterm infants and infants with low birth weight are increasing. In particular, the birth rate of late-preterm infants, whose gestational age is over 34 weeks and 0 days but under 36 weeks and 6 days, is markedly high [1]. Late-preterm infants’ gestational age is close to that of full-term infants, and until recently they were called “near-term infants” and provided with medical treatment meant for full-term infants based on the assumption that they would experience few health problems after birth [2]. Although late-preterm infants are born premature, parents and medical staff often do not realize that they are less neurologically and physiologically mature than full-term infants [3]. Accordingly, late-preterm infants are usually discharged early with the mother after observation in the neonatal room (NR) for a relatively brief period [4]. Compared with full-term infants, however, late-preterm infants show a higher rate of morbidities including infant respiratory distress syndrome and hyperbilirubinemia [4,5], and also often experience hypothermia, jaundice, breastfeeding difficulties, and hypoglycemia [6]. A study conducted in South Korea reported that problems such as hypoglycemia, breathing difficulties, and delayed breastfeeding initiation were significantly more common in late-preterm infants than in full-term infants [7].
Breast milk is the best source of nutrition for late-preterm infants, but they are often difficult to breastfeed because they frequently become sleepy and display week sucking power [8]. Although it may seem easy to breastfeed late-preterm infants because they appear similar to full-term infants, they have difficulty coordinating the essential components of successful breastfeeding (sucking, breathing, and swallowing) [9]. Therefore, breastfeeding initiation is delayed and the duration of breastfeeding sessions is short [10]. Breastfeeding difficulty is a primary cause of inadequate weight gain after birth [8]. In the hospital, babies can be fed with formula, provided with enteral feeding, or administered intravenous injections [8]. However, if late-preterm infants are cared for in the same way as their full-term counterparts after discharge, the risk of insufficient nutrient intake increases [11] and growth may be impaired. Accordingly, mothers of late-preterm infants should be fully educated on breastfeeding. Breast milk facilitates the growth of butyric acid bacteria and Lactobacillus in the intestines and decreases the risks of sepsis and necrotizing enterocolitis [8]. The main reasons for hospital readmission in late-preterm infants include breastfeeding difficulties, jaundice, and infection [6]; therefore, effective breastfeeding is expected to lower readmission rate in this population.
Premji et al. [12] observed that mothers of late-preterm infants displayed low parenting confidence until 6~8 weeks after delivery. Parenting confidence is essential for parents to successfully perform their roles [13]. Hence, nurses should educate mothers of late-preterm infants on the characteristics and behaviors, breastfeeding methods, and health problems specific to these infants in order to increase their parenting confidence [12]. A study found that mothers of late-preterm infants admitted to the neonatal intensive care unit (NICU) felt more confident when they were provided with an opportunity to learn about the basics of infant care such as breastfeeding, changing diapers, measuring body temperature, and bathing [12]. Educating mothers of preterm infants on infant care during the hospital stay is linked to better infant health and mother-infant interaction outcomes [6]. Furthermore, a higher level of parenting confidence in mothers increases infant care ability and self-regulation, reduces stress, and consequently promotes infant health and wellbeing [12].
The readmission rate after discharge is higher in late-preterm infants than in full-term infants, and common reasons for readmission include breastfeeding difficulties, jaundice, breathing difficulties, and infection [14]. In a study conducted in South Korea, breastfeeding difficulties and a brief observation period in the NR were identified as risk factors for readmission in late-preterm infants [7]. If parents of late-preterm infants are not adequately educated about breastfeeding during the initial hospital stay, inadequate weight gain can be another reason for readmission [11]. Therefore, to decrease the readmission rate in late-preterm infants, the breastfeeding rate should be increased through sufficient education, practice, and reinforcement. In addition, parenting confidence must be enhanced through education and support with respect to late-preterm infants’ characteristics and health management needs.
Interventional studies targeting stress, parenting confidence, breastfeeding, mother-infant attachment, anxiety, and depression in mothers of preterm infants have been conducted using workbook programs [15], booklets [16], systematic information [17], and empowerment programs [18]. However, most have focused on mothers of preterm infants under 37 weeks of gestational age and with a birth weight below 2,500 g. The discharge education provided to mothers of preterm infants, including those with a birth weight below 1,500 g, focuses on preterm infants’ characteristics, emergency coping skills (cardiopulmonary resuscitation), oxygen therapy, enteral feeding, and the use of monitors [15-18], which is inappropriate for late-preterm infants.
Accordingly, the present study aimed to develop an infant care education program for mothers of late-preterm infants with a focus on breast milk management including breastfeeding [9], and the prevention and management of problems that frequently occur in late-preterm infants [3-6]. An additional objective was to examine the intervention program’s effects on breastfeeding rate and parenting confidence in mothers, and on growth and readmission rate in infants.
1. Study Hypotheses
∙ Hypothesis 1: The parenting confidence score will differ between the experimental and control groups across postintervention time points.
∙ Hypothesis 2: After the intervention, the breastfeeding rates will differ between the experimental and the control groups.
∙ Hypothesis 3: Late-preterm infants' growth levels will differ between the experimental and the control groups across post-intervention time points.
∙ Hypothesis 4: After the intervention, late-preterm infants’ readmission rates will differ between the experimental and control groups.
METHODS
1. Study Design
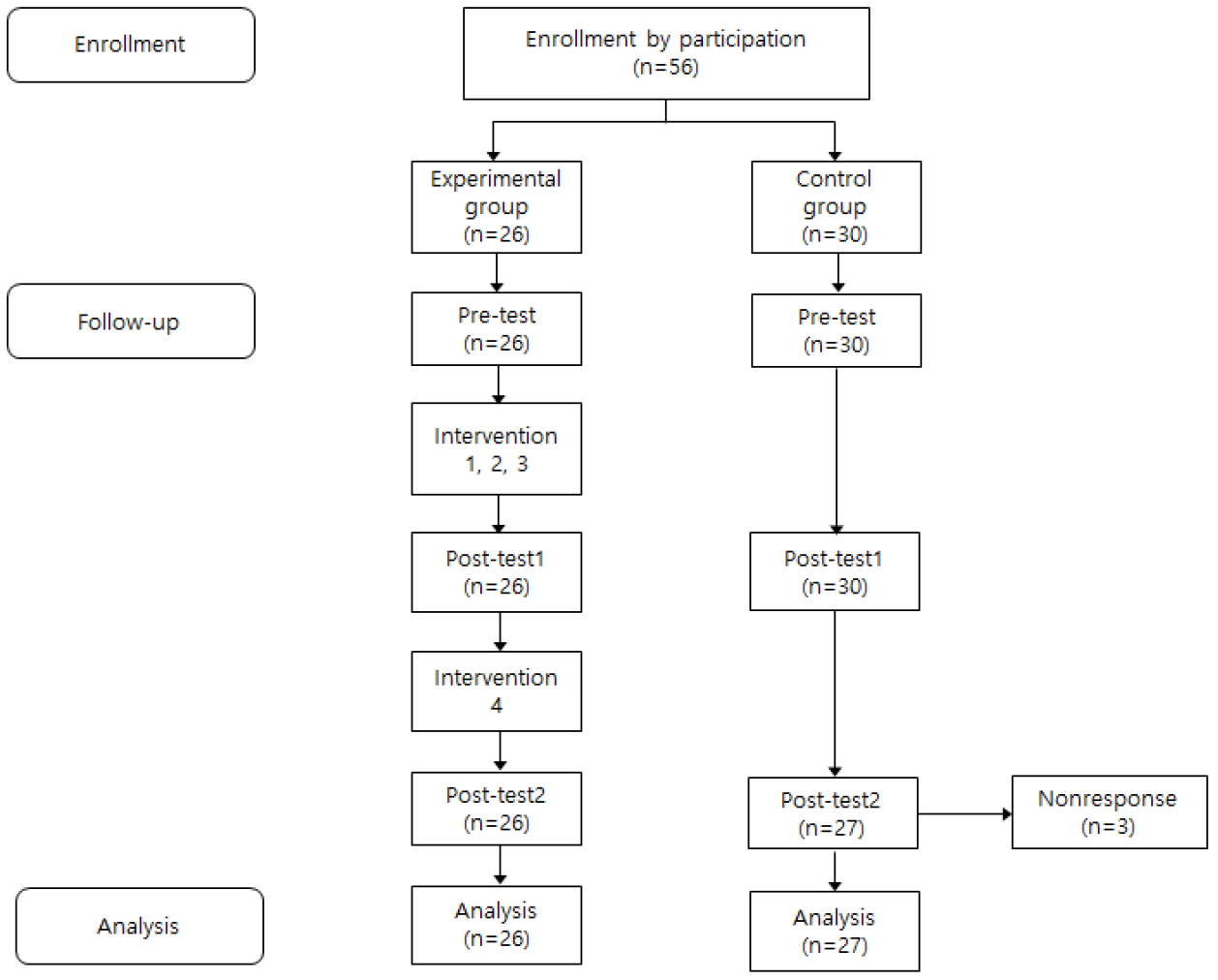
This quasi-experimental study employed a nonequivalent control group non synchronized design (Figure 1).
2. Participants
The participants were mothers who voluntarily agreed to participate in the study after receiving a comprehensive explanation of its purposes and procedure, together with their late-preterm infants admitted to the NICU of a general hospital in B city. The selection criteria for infants were as follows: gestational age over 34 weeks and 0 days but under 36 weeks and 6 days, absence of congenital disorders, and absence of severe complications. The selection criteria for mothers were as follows: absence of postpartum complications, no problem visiting the NICU, the ability to read and comprehend Korean, and provision of consent for follow-up home visits.
G*Power 3.1.6 was used to estimate the appropriate sample size. The minimum required sample size was 28, under the assumptions of a medium effect size (.25) for the F-test (repeated-measures analysis of variance [ANOVA]), a significance level of .05, a power of .80, two groups, three repeated measures, and a repeated-measures correlation of .50. The drop-out rate was assumed to be approximately 50% on the basis of follow-up until a month post discharge, and the required sample size was accordingly determined to be 60, with 30 mothers each in the experimental and control groups. A total of 56 women were recruited: 30 in the experimental group and 26 in the control group. After excluding three women from the control group because they were lost to follow-up after discharge, the final study sample comprised 53 women: 26 in the experimental group and 27 in the control group.
3. Research Instruments
1) Demographic characteristics
Eleven items were used to collect data on demographic characteristics, including age, educational level, occupation, religion, monthly household income, delivery method, and obstetric history (for mothers) and gestational age, sex, birth order, and length of hospital stay in days (for infants).
2) Parenting confidence
To assess parenting confidence, the instrument that Park [19] translated into Korean and modified to fit the South Korean context based on the 13 items of Pharis's Self-confidence Scale was used. The instrument consists of a total of 38 items across 6 domains: wellbeing and safety, infant behavior, breastfeeding, hygiene, bathing and diaper changing, and health and illness. The items are scored on a 5-point Likert scale from 1 (“not confident”) to 5 (“extremely confident”). The total scores range from 38 to 190, and higher the scores, indicate higher parenting confidence. Cronbach’s ⍺ was .95 in Park’s study [19], and .96 in the present study. Although the original developer and translator were contacted multiple times for permission to use the instrument, neither responded.
3) Breastfeeding rate
To evaluate the breastfeeding rate, the World Health Organization’s nutrition classification system was used [20]. In this system, stage I is defined as 100% breastfeeding, stage II as more breastfeeding than formula feeding, stage III as 50% breastfeeding and 50% formula feeding, stage IV as more formula feeding than breastfeeding, and stage V as 100% formula feeding. In the present study, with reference to Jeong [21], stages I through IV were defined as breastfeeding and stage V as formula feeding, and feeding type was examined on the day of discharge and a month after discharge.
4) Growth of late-preterm infants
To assess the growth of late-preterm infants, weight, height, and head circumference were measured at birth, discharge, and a month after discharge. Weight was measured with a scale (BS-203, Bodycom, China) tared to 0. Babies were weighed twice with their diaper and clothing removed, and their average weight was computed. Height and head circumference were measured in centimeters using a tape measure (Rollfix, Hoechstmass, Germany). Height was measured from head to toe, with the baby lying straight in the supine position, and was computed as the average of two measurements. Head circumference was measured by wrapping the tape measure around the widest circumference covering the area above the eyes through the auricle and the occipital protuberance, and the average of two measurements was recorded as the head circumference.
4. Study Procedure
1) Program development
To develop the program, multidisciplinary guidelines for the care of late-preterm infants [22], ABM clinical protocol #10(breastfeeding the late-preterm infant) [23], and a previous study on late-preterm infants [11] were referred to. Finally, a small booklet was produced to provide mothers of late-preterm infants with practical help in caring for the baby.
The booklet was composed of sections regarding late-preterm infants' characteristics, health problems, growth, breastfeeding, and home care. It emphasized that late-preterm infants are preterm infants, and explained that they can easily experience breathing difficulties, hypoglycemia, infection, breastfeeding difficulties, and jaundice. As late-preterm infants often become sleepy during breastfeeding and have weak sucking power, methods of waking up a sleepy baby for breastfeeding and various postures to support the baby during breastfeeding were introduced. The booklet was designed to be portable so that mothers could use it not just in the three intervention sessions but also in the maternity room during their hospital stay and at home as required. After the baby was discharged, the booklet was also used to educate mothers on infant care at home, hospital visits, and vaccinations. A feeding diary was included in the booklet such that mothers could maintain feeding-related records and records on the volume and pattern of urination and bowel movements. To facilitate a visual understanding, PowerPoint slides were created to summarize the contents of the booklet.
The educational materials were developed in consultation with a pediatric nursing professor and three nurses with over 10-years of experience in NRs. Prior to the main study, a pilot study was conducted with three mothers of late-preterm infants to evaluate the program contents and assess mothers’ understanding and interest level. The pilot study did not indicate the need for any revisions. A summary of the late-preterm infant care education program is presented in Table 1.
2) Experimental treatments
The late-preterm infant care education program was administered by the present researcher. The first, second, and third interventions were performed in one-on-one meetings using the booklet and PowerPoint slides in the breastfeeding room in the NR or in the maternity room, before the baby was discharged. Immediately after each intervention session, mothers were encouraged to ask questions about what they wanted to know or did not fully understand. The fourth intervention was performed using a telephone and social networking service (SNS) after discharge, once weekly, to encourage and support the mothers through counseling.
(1) First intervention
The first intervention was performed for 60 minutes within a day or two of the baby being born, either in the maternity room or the breastfeeding room in the NR depending on the mother’s health status after delivery. Before the intervention, the researcher introduced herself and provided an overview of the education. Then, she explained late-preterm infants' characteristics, health problems, common reasons for readmission, and growth patterns using the booklet and PowerPoint slides. Mothers were also educated on the advantages of breastfeeding and how to identify infants’ signals for feeding. If breastfeeding was deemed possible given the baby’s health status, mothers were given instructions regarding how to facilitate latching. Mothers were instructed to use the booklet and repeat what they had learned, after returning to the maternity room from the NR.
(2) Second intervention
The second intervention, which lasted 30 minutes and made use of PowerPoint slides, was performed 3~4 days after childbirth in the NR’s breastfeeding room. The contents included further details on breastfeeding. Since the production of breast milk increases 3~4 days after childbirth, during the second intervention, mothers were instructed to actually breastfeed the baby and taught about the proper breastfeeding posture, if possible given the health status of the mother and infant. As the length of hospital stay is generally shorter for late-preterm infants than for preterm infants whose gestational age is lower than 34 weeks, mothers were encouraged to have the baby latch onto the breast at will. Waking up the sleepy baby during breastfeeding and checking to see whether or not the baby had enough breast milk were emphasized. Mothers were shown various breastfeeding postures, including the football hold for babies with weak sucking power. Mothers were also shown how to prevent breast engorgement and cope with mastitis, which can occur with increased production of breast milk.
(3) Third intervention
The third intervention, which made use of the booklet, was performed for 40 minutes a day before the baby was discharged. The contents included home care after discharge, observation of bowel movements, and maintaining a feeding diary. Mothers were instructed to use the feeding diary to record whether the baby was breastfed the duration and amount of feeding, and the occurrence of urination and bowel movements.
(4) Fourth intervention
The fourth intervention was performed once every week for 1 month after discharge, via telephone and SNS, to assess whether the baby was breastfed, the duration and amount of feeding, and the daily frequency of urination and bowel movements. Mothers were encouraged to ask questions regarding infant care and to express any difficulties they were experiencing when caring for the baby, while being provided with supportive nursing care. Additionally, mothers were encouraged to contact the researcher by telephone or SNS to ask questions at any time.
The control group was provided with conventional education by the nurse in charge. At the time of admission, the nurse in charge used a one-page leaflet to teach mothers in the control group about storing, freezing, and thawing breast milk. Then, a day or two before discharge, in the NR, the nurse provided general instructions on latching onto the breast and bottle-feeding. On the day of discharge, mothers were given a one-page discharge leaflet and provided with conventional discharge education for 10~20 minutes.
3) Data collection
The data collection period was September 2014 through July 2015 for the control group, and August 2015 through June 2016 for the experimental group. To prevent treatment contamination, the experimental group received the intervention after the conclusion of data collection from the control group.
A pre-intervention survey was conducted with mothers of late-preterm infants who visited the NR 1~2 days after the baby was admitted. In both the experimental and control groups, data were collected on demographic characteristics, childbirth, and parenting confidence. The survey took 15~20 minutes to administer. During the pre-intervention survey, the baby’s weight, height, and head circumference were each measured twice by the researcher and the mean value was recorded. Subsequently, the control group received conventional discharge instructions from the nurse in charge of the baby, whereas the experimental group received the intervention.
The first post-intervention survey was conducted on the day of discharge in both the experimental and control groups. The parenting confidence scale was administered and whether the baby was being breastfed was examined. Additionally, the baby's weight, height, and head circumference were measured by the researcher. The second post-intervention survey was administered during a home visit one month after discharge in both groups. Mothers were notified two to three days before the home visit to obtain consent. During the home visit, the researcher used a self-report questionnaire to collect data on mothers' parenting confidence, whether they were breastfeeding the baby, and whether the baby had been readmitted, and measured the baby's weight, height, and head circumference using the same measurement tools as mentioned above.
5. Ethical Considerations
This study was approved by the Institutional Review Board (IRB) (H-1406-004-018). As recruiting participants proved difficult, the study period was extended with IRB approval. The participants were mothers of late-preterm infants who voluntarily agreed to participate in the study. The written informed consent form provided a description of the study and its purposes and, procedures as well as the potential benefits and drawbacks of participation. Participants were also informed of the confidentiality of their data and their rights to withdraw from study at any time. They were given a small gift for their participation.
6. Data Analysis
The data were analyzed using SPSS for Windows version 22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to examine demographic characteristics, parenting confidence, weight, height, and head circumference. Homogeneity of the experimental and the control groups was tested using the t-test, χ2 test, and Fisher's exact test, and the hypotheses were tested with the χ2 test, Fisher exact test, and repeated measures ANOVA. If a time-by-group interaction was significant, a post-hoc test was performed to identify the time point when the two groups differed from each other. To reduce type 1 error, the significance level was corrected to .017 using the Bonferroni method.
RESULTS
1. Homogeneity Testing of Demographic and Outcome Variables
The results of the homogeneity testing of demographic and outcome variables are presented in Table 2. Mothers’ parenting confidence, and late-preterm infants’ weight, height, and head circumference at birth were not statistically significantly different between the groups, thus confirming homogeneity in the outcome variables. The Shapiro-Wilk test was conducted to test the dependent variables for normality, and it was confirmed that parenting confidence, as well as the infants’ weight, height, and head circumference at birth, were all normally distributed.
2. Testing for Program Effects
To test hypothesis 1 (that the parenting confidence score will differ between the experimental and control groups across post-intervention time points) repeated-measures ANOVA was conducted. As the Mauchly test of sphericity showed that the sphericity assumption was not met (W=.676, p<.001), the value of epsilon was corrected using the Greenhouse-Geisser method. The Shapiro-Wilk test demonstrated that parenting confidence met the normality assumption (W=.973, p=.281).
For parenting confidence, the time-by-group interaction was significant (F=4.17, p=.029), and hypothesis 1 was therefore supported (Table 3). To test between-group differences at each time point, the independent t-test was were conducted, with the following results. The score immediately after intervention was 127.50 in the experimental group and 110.33 in the control group (a difference of 17.17 points), and the difference was significant (t=2.66, p=.010). The score at 1 month after discharge was 140.15 in the experimental group and 123.40 in the control group (a difference of 16.75 points); again, the between-group difference was significant (t=2.92, p=.005). To test for within-group differences across time, the paired t-test was conducted. In the experimental group, the parenting confidence score increased by 14.54 points and 27.19 points immediately after the intervention and 1 month after discharge versus prior to intervention, respectively (t=2.81, p=.010; t=4.95, p<.001). In the control group, while the score did not statistically significantly change from before to immediately after the intervention, a statistically significant change was observed from before the intervention to 1 month after discharge (t=5.12, p<.001) (Table 3).
To test hypothesis 2 (that after the intervention, the breastfeeding rates will differ between the experimental and control groups) the χ2 test was performed. While there was no significant between-group difference on the day of discharge, the breastfeeding rates 1 month after discharge (73.1% and 40.7% in the experimental and control groups, respectively) were statistically significantly different between the groups (t=5.64, p=.018). Hence, hypothesis 2 was supported (Table 4).
To test hypothesis 3 (that late-preterm infants’ growth levels will differ between the experimental and the control groups across post-intervention time points) repeated measures ANOVA was performed. As the Mauchly test did not confirm sphericity in the dependent variable, the value of epsilon was corrected using the Greenhouse-Geisser method. The Shapiro-Wilk normality tests confirmed that infants’ weight (W=.963, p=.097), height (W=.985, p=.737), and head circumference (W=.976, p=.350) were all normally distributed. Repeated measures ANOVA showed that weight, height, and head circumference all increased over time, but the time-bygroup interaction was not significant for weight (F=2.24, p=.124), height (F=2.13, p=.139), or head circumference (F=0.24, p=.724). Thus, hypothesis 3 was rejected (Table 3).
In testing Hypothesis 4,(that after the intervention, late-preterm infants’ readmission rates will differ between the experimental and control groups) it was observed that no infant in the experimental group was readmitted after discharge, while this number was one (3.7%) in the control group. Thus, the readmission rates were not statistically significantly different between the groups, and hypothesis 4 was rejected (Table 4).
DISCUSSION
This study was conducted to develop an infant care education program for mothers of late-preterm infants and to investigate its effects on parenting confidence and breastfeeding rate in mothers, and on growth and readmission rate in infants.
In the experimental group, the parenting confidence score was 112.96, 127.50, and 140.15 during the hospital stay, at discharge, and 1 month after discharge, respectively, indicating that there was a significant increase over time in this group compared with baseline, and these scores were significantly higher than those of the control group. This finding is consistent with the results of several studies [16-18] reporting that after an educational intervention, the parenting confidence of mothers of preterm infants improved. Parenting confidence refers to mothers’ competence in rearing a baby and their ability to recognize the baby’s needs [17], and it is acquired by repeatedly practicing specific infant-care activities [16]. Breastfeeding difficulties in late-preterm infants can decrease mothers’ confidence [12], and it is speculated that mothers' parenting confidence was enhanced in this study because the focus of the program was breastfeeding education and they were repeatedly taught how to store breast milk at home even before discharge.
Booklets involve low production costs, are convenient to carry, and can be used anywhere without the need for any special tools [24]. A study that investigated the effect of radiation safety management education for intensive care unit nurses also, reported that the educational effect of face-to-face sessions with a small number of learners using a booklet was greater than that of self-directed learning using a video [24]. It is speculated that in this study, since it was easy to carry the booklet and peruse it at will, the mothers were able to review the information on infant care at any time, which contributed to the improvements in their parenting confidence. Learning is much more effective when the learner actively participates in the learning process, as opposed to when learning materials are delivered unidirectionally [25]. Hence, it is believed that in the present study, the positive educational effect was a result of giving the mothers increased opportunities to practice what they had learned and providing appropriate feedback to their responses after a face-to-face session using the booklet and PowerPoint slides.
Jang [26] stated that to improve mothers’ parenting confidence, providing them with an intervention continuing from the time of the baby’s hospitalization to after discharge is more effective, than intervening only while the baby is in the hospital or only after discharge. Accordingly, the mothers in the present study were contacted through SNS once a week until 1 month after discharge to give them an opportunity to ask any questions that might have arisen during the process of caring for the baby. They commonly had questions on daily feeding volume, how to cope with vomiting after a feeding, abnormal breathing sounds, whether to breastfeed when the baby was having diarrhea, changes in bowel movements, abdominal distension, and sleeping problems. The mothers were encouraged to express the difficulties they experienced in caring for the baby and were listened to with empathy and encouragement. They were also told about other mothers' experiences for emotional support. In contrast with most previous studies [15-18] in which one-time telephone counseling was provided a week or a month after discharge, in the present study counseling was regularly provided via telephone and SNS once a week until 1 month after discharge, which is believed to have been helpful in enhancing parenting confidence.
The breastfeeding rates at 1 month after discharge were 73.1% in the experimental group and 40.7% in the control group. While this finding is in line with a previous study [15] reporting a higher breastfeeding rate in participants who received a workbook program intervention, the rate was much higher in this study. The breastfeeding experiences of mothers of late-preterm infants include challenges such as having the baby latch onto the breast and supplying breast milk, insufficient production of breast milk after hospital discharge, and a sense of failure [10]. To promote breastfeeding, the infant care education program developed in this study included practicing breastfeeding in the first and second intervention sessions. In addition, mothers were repeatedly educated via telephone and SNS every week until a month after discharge to evaluate whether the baby was properly breastfeed and to assess the amount and duration of feedings, and were encouraged and supported when breastfeeding was difficult and the baby did not want to eat. All this supportive nursing is believed to have been effective.
The current findings strongly align with those of a study by Jang and Kim [27]. In their study, mothers were educated on breastfeeding from immediately after delivery until discharge and received telephone counseling once a week after discharge until 1 month after delivery, and while it was found that at discharge, the breastfeeding rate was not statistically significantly different between the experimental and control groups, at 1 month after delivery the rate was 75.0% in the experimental group and 26.3% in the control group, showing a significant between-group difference. However, in the study of Jang and Kim [27], the participants were mothers of healthy babies with a gestational age between 37 and 42 weeks and a birth weight over 2,500 g. Thus, the program developed in this study may be the first to show the effect of infant care education on the breastfeeding of late-preterm infants. The findings also suggest that the breastfeeding rate may increase if mothers try to breastfeed the baby even only once during a short hospital stay and are repeatedly supported and encouraged after discharge.
With respect to the effect of the infant care education program on the growth of late-preterm infants, infants' weight, height, and head circumference increased over time in both the experimental and control groups, but did not show statistically significant between-group differences. As late-preterm infants have weak sucking power and are not coordinated in the oral movements of sucking and swallowing, they are at risk for dehydration and insufficient caloric intake, which can lead to weight loss [11]. Hence, in the program presented in this study, mothers were encouraged to practice breastfeeding and to continue breastfeeding after discharge, and the volume of food intake was assessed by instructing them to record feeding amounts and bowel movements. Nonetheless, the growth of the infants did not show a significant between-group difference, and the reason is speculated to be that the follow-up period of 1 month post-discharge was too short. Jang and Kim [27] stated that breast milk and baby formula were not associated with differing growth levels, based on the finding that while breastfeeding rates differed between mothers of full-term infants provided with breastfeeding education and support and the control group, there was no between-group difference in the growth of infants. In the past, it was generally believed that breast milk slows growth. More recently, however, it was pointed out that this belief, which stemmed from using infants fed with prescribed formula as the reference group, is erroneous [28]. In addition, several studies have demonstrated that there is no difference in growth between babies fed with breast milk and those fed with formula [27,28]. Therefore, nurses should emphasize the immunological and emotional advantages of breastfeeding, and should ensure that mothers do not stop breastfeeding too early if the baby grows slowly.
The experimental and control groups did not show statistically significant differences with regard to infants’ readmission rates. None of the infants in the experimental group was readmitted within a month after discharge and only one (3.7%) in the control group was readmitted owing to enteritis. It is speculated that the null finding was due to a small sample size, as the study was conducted at a single institution, and because too short a follow-up period was used (only 1 month after discharge). Considering Kim’s study [29], wherein 113 (83.7%) of 135 late-preterm infants who were readmitted had jaundice and the next most common reason for readmission was diarrhea (n=9, 6.7%), mothers should be educated on common symptoms and reasons for readmission in late-preterm infants and hand-washing and infection prevention should be stressed. Although statistical significance was not observed in this study, the infant in the control group who was readmitted was fed with formula, while no infants fed with breast milk were readmitted. Preterm infants are compromised in terms of their antioxidative ability, and breast milk has antioxidant properties that help neutralize oxidative stress [11]. Thus, effective breastfeeding is expected to help strengthen the immune system, including the prevention of enteritis in late-preterm infants.
To summarize the findings, the infant care education program increased mothers’ understanding of late-preterm infants and enhanced parenting confidence, while simultaneously encouraging and supporting breastfeeding. Unlike other studies, the program in the present study focused on late-preterm infants, stressed the importance of breastfeeding, provided the mothers with opportunities to practice breastfeeding during their hospital stay, and regularly provided weekly telephone and SNS counselling even after discharge.
However, the study has the following limitations. First, it was difficult to recruit mothers of late-preterm infants and there was a nearly 1-year gap in the data collection period for the experimental and control groups, making it difficult to generalize the findings. Thus, the study should be replicated to confirm its findings. Second, the growth and readmission rates of late-preterm infants were examined only until 1 month after discharge; they were not followed up over a long period. Despite these limitations, this study is of significance in that it focused on late-preterm infants, who are less mature than full-term infants, and provided infant care education targeting specifically late-preterm infants, as opposed to education uniformly given to all mothers of preterm infants. By emphasizing breastfeeding education during the hospital stay and providing regular education and counseling after discharge, the intervention described in this study is expected to be useful for improving mothers’ understanding of late-preterm infants and providing them with practical help in childbearing.
CONCLUSION
This quasi-experimental study was conducted to develop a late-preterm infant care education program and investigate its effects in order to provide mothers with practical information and help with child-rearing. The effects of the program on mothers’ parenting confidence and breastfeeding rate and on infants' growth and readmission rate were examined, and it was found that the breastfeeding rate was significantly higher in the experimental group than in the control group. Accordingly, it is concluded that the program developed in this study, which provided mothers with information on late-preterm infants and regular education and counseling even after discharge, was useful for improving parenting confidence and breastfeeding rates, and that the quality of preterm-infant nursing will be enhanced by developing new nursing interventions.