INTRODUCTION
1. Need for Study
The number of births has steadily decreased in Korea, from 465,900 births in 2008 to 326,800 births in 2018. However, the proportion of preterm births has increased from 5.5% of births (25,655 cases) in 2008 to 7.8%(25,202) in 2018 [1]. Preterm or premature infants born at less than 37 weeks of gestation are likely to be at a greater risk of morbidity and mortality than full-term infants [2].
Late preterm infants (LPIs), born between 34 weeks and 36 weeks of gestation [3], are more likely than term infants to have respiratory distress, feeding difficulties, hyperbilirubinemia, hypothermia, hypoglycemia, and a septic workup just after birth [4,5]. In particular, LPIs cared for in a neonatal intensive care unit (NICU) were more likely to have those problems than LPIs initially cared for in a nursery [4]. Neonatal jaundice, dehydration, and poor weight gain are major health problems among breastfed LPIs after discharge [6]. In addition, LPIs who are breastfed are more likely to be readmitted due to neonatal jaundice or infections than term infants who are breastfed [5]. Hospital readmission related to neonatal jaundice and poor feeding is almost twice as common among breastfed LPIs as among non-breastfed LPIs, and LPIs are at a greater risk for breastfeeding-associated morbidity and poor breastfeeding establishment [7]. Therefore, improving breastfeeding support and education is likely to reduce neonatal jaundice and breastfeeding-associated hospital readmission [8].
Breastmilk jaundice occurs when bilirubin levels are 12 mg/dL or higher [9]. The condition is caused by enterohepatic circulation issues, not by any specific ingredient in human milk. In other words, decreased breastmilk intake slows bowel movements and causes slower bilirubin elimination, aggravating jaundice. This is often referred to as breastfeeding failure jaundice [10]. However, in clinical settings, many neonatologists may encourage mothers to withhold breastfeeding and substitute breastmilk with infant formula when breastfeeding jaundice occurs in LPIs at a certain period postpartum. In addition, almost half of LPIs were discharged with advice to be fed with infant formula [11].
The American Academy of Pediatrics [12] recommends exclusive breastfeeding for the first 6 months, as breastmilk has been proven to be the most ideal nutritional source for the growth and development of newborns. However, as the breastfeeding rate of 63.8% at 1 month postpartum in LPIs is lower than the rate of 76.5% in term infants [13], LPIs are considered to be a population at an elevated risk for shortened breastfeeding duration, underscoring the need to develop specific breastfeeding support and education [13]. In particular, the breastfeeding rate at 1 month post-discharge in Korean LPIs (42.5%) is lower than that of any other country [14]. As an association between lower breastfeeding rates and late preterm birth has been reported, high hospital support for breastfeeding is thought to be likely to increase the prevalence of exclusive breastfeeding. However, just 16.4% of LPIs received such support, compared with 30.7% of term infants [15].
The late preterm breastfeeding promotion interventions conducted in previous studies involved skin-to-skin contact to simulate breast milk production just after birth, cup feeding and triple feeding instead of bottle-feeding to improve breastfeeding, and a family care program recommending rooming-in in the NICU to facilitate breastfeeding by providing the mother with unrestricted access to the baby [2]. These interventions were primarily implemented in hospitals during the LPIs' hospital stay and discontinued after discharge.
In contrast, the breastfeeding coaching program (BCP) in this study was a repetitive, community-based intervention to establish exclusive breastfeeding for LPIs for 1 month after discharge to compensate for the known limitations of previous interventions. This program consisted of web-based breastfeeding education with practical lactation support, focusing on relatively unhealthy LPIs discharged from the NICU. The main goal of the BCP was to successfully transit from mixed feeding (combination of breastfeeding and formula feeding) at discharge to exclusive breastfeeding at 1 month after discharge. A further motivation for the BCP was that mothers of LPIs admitted to the NICU have little experience of feeding their infants at the breast and have expressed a lack of breastfeeding education and support [15]. Moreover, the hospital readmission rates for LPIs can be reduced by 50% through breastfeeding education [16].
Thus, the effects of a BCP for LPIs discharged from the NICU on breastfeeding rate, LPIs' growth, neonatal jaundice, and neonatal morbidity during 1 month after discharge were investigated. This study aimed to determine the influence of the BCP on the breastfeeding rate and neonatal morbidity in LPIs.
METHODS
1. Study Design and Participants
This was a non-randomized quasi-experimental study with a time series design that investigated the effects of a BCP for mothers of LPIs on breastfeeding rates, LPIs' growth, neonatal jaundice, and neonatal morbidity. An article on the impact of the BCP on LPIs' growth and neonatal jaundice is being processed for publication in a different journal, and this is a separate study of the influence of this program on breastfeeding rates and neonatal morbidity for 1 month after LPIs' hospital discharge.
The required sample size was calculated as 36 using PASS 2008 (NCSS LLC, Kaysville, UT, USA), with a significance level of .05, a statistical power of .08, four repeated measurements and two groups (experimental and control) with breastfeeding rates of 55% and 25%, respectively [17]. Forty LPIs were selected as the final sample, considering a possible withdrawal rate of 10%.
The participants were 40 LPIs and their mothers in a NICU at a university hospital located in Daegu, South Korea. The mothers indicated that they understood the purpose of the study and consented to participate. The inclusion criteria were: a) mothers who did not have previous breastfeeding experience and intended to breastfeed; b) mothers who consented to weekly home visits during the study period; c) LPIs with a 1-minute Apgar score ≥5 and/or a 5-minute APGAR score ≥7; and d) LPIs who did not have any hemorrhagic problems. The exclusion criteria were: a) LPIs in whom oral feeding was delayed for more than 2 day due to respiratory problems or surgery; and b) LPIs in the NICU who were readmitted with medical issues after being discharged.
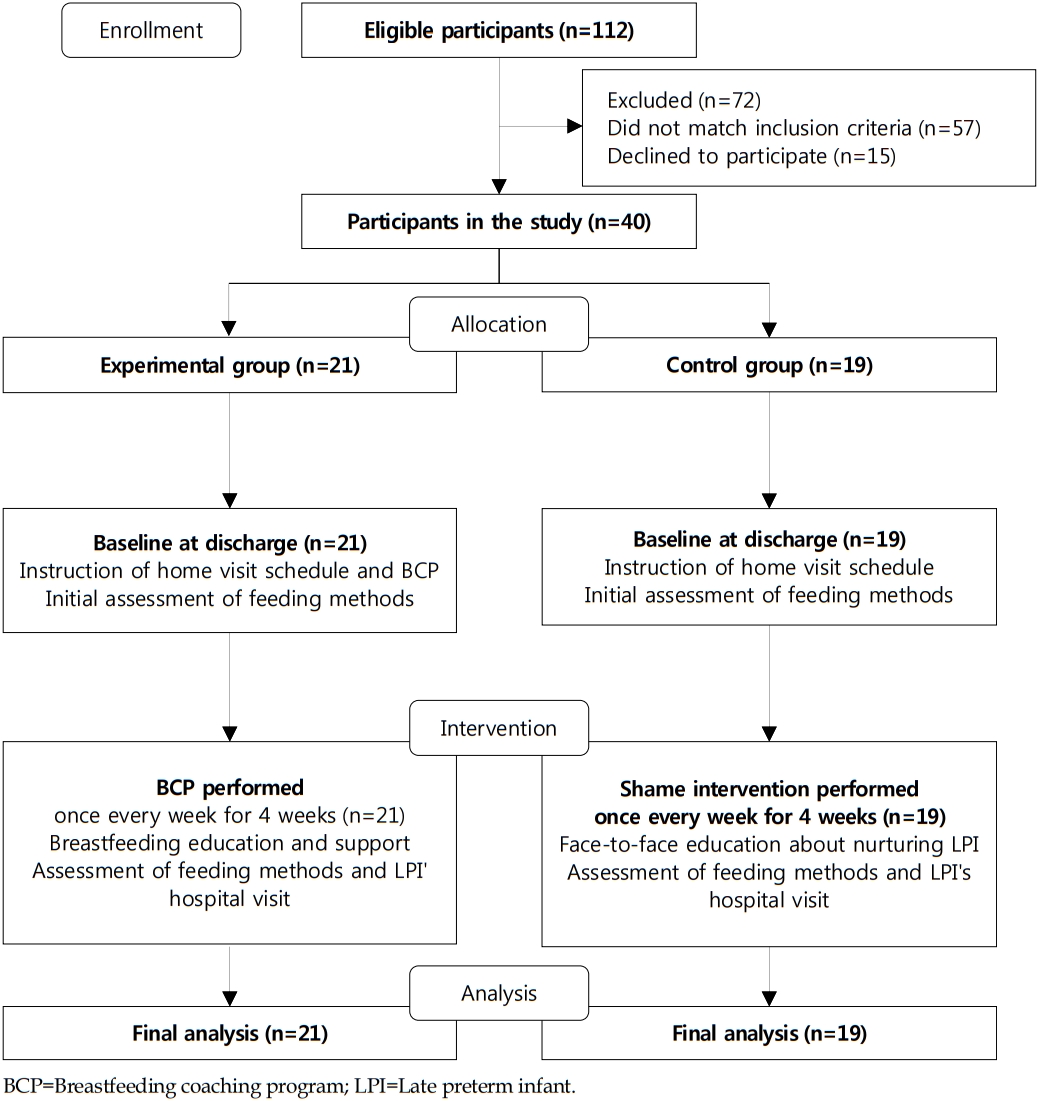
The participants were first allocated to the control group,The participants were first allocated to the control group, and then consecutively allocated to the experimental group to prevent contamination between participants. The number of participants allocated to the experimental and the control groups was 21 and 19, respectively (Figure 1).
2. Intervention Program
The BCP used a modified version of the breastfeeding support program (BSP) developed by Jang and Hong [17] for LPIs discharged from the NICU (Table 1). This program consisted of web-based breastfeeding education and practical breastfeeding support, and was provided for mothers in the experimental group on a weekly basis through a researcher's home visit. This website was available only when a researcher permitted mothers to access it.
On the day of discharge, mothers in the experimental group were given the home visit schedule and the webpage where the lactation education was available. On the first and second week after discharge, the researcher provided breastfeeding education through the web after assessing the infants' suck-swallow-breathe coordination and oral-motor skills during the LPIs' feeding. Most of the LPIs were still not ready to directly feed from their mothers' breasts due to their physical and neuromuscular immaturity; therefore, the sessions were focused on regular pumping to stimulate breastmilk production. However, some mothers whose LPIs had sufficient oral-motor skills to feed were encouraged to latch at least once or twice a day. On weeks 3 and 4, the researcher assessed the mother-infant dyad's feeding skills and helped the infants latch properly by correcting their positioning. Mothers were also taught ways of checking whether their babies were receiving enough milk given the difficulty in knowing exactly how much the infant consumed through direct nursing.
The control group was informed of the weekly home visit schedule upon discharge. At the following weekly visits, nurturing guidance for LPIs was provided by the same researcher. Questions on caring for LPIs, including the use of nutritional supplements such as iron, the outpatient visit schedule, and behavioral phenomena such as startle reflex, as well as breastfeeding-related questions, were answered with appropriate responses, but no practical support was provided to encourage breastfeeding. The average visit was between 1 hour and 1.5 hours in both group.
The BCP for the experimental group and nurturing guidance for the control group were provided through weekly home visit by the same researcher, who has an International Board Certified Lactation Consultant credential.
3. Feeding Methods and Neonatal Morbidity
Feeding methods were defined as follows: breastfeeding, mixed feeding, and formula feeding. Breastfeeding was defined as direct feeding at the breast or bottle-feeding with pumped breast milk. Mixed feeding referred to a combination of breastfeeding and supplementation with infant formula. Formula feeding was defined as being exclusively formula-fed.
Based on a study conducted by Tomashek et al. [5], neonatal morbidity was defined as any health condition or illness that required hospital readmission or an observational hospital stay in the first month of life. An observational hospital stay was a hospital outpatient visit or an emergency room visit lasting less than 24 hours. When health issues in LPIs were reported, transcutaneous bilirubin levels and body weight were checked to evaluate the infants' condition.
4. Data Collection
Data were collected at a university hospital in Daegu, South Korea, which operates a nationally designated NICU center with 35 beds, between June 2017 and May 2018. Participants in the control group were collected from June to October 2017 and those in the experimental group, from November 2017 to May 2018. A nurse working as a lactation specialist in that hospital gathered the demographic and clinical characteristics of LPIs and feeding methods in the NICU from their electronic medical records on the day before discharge and contacted the researcher. The researcher checked the LPIs' feeding methods and whether they had experienced any health problems requiring a hospital outpatient visit or an emergency department visit once a week, from week 1 to week 4 after discharge.
5. Statistical Analysis
Data were analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics, the t-test, and the x2 test were used to compare the clinical characteristics of the two groups of LPIs. Feeding methods each week and neonatal morbidity were compared between the two groups using the x2 test. Feeding methods and neonatal morbidity were analyzed using logistic regression to adjust for clinical characteristics that were significantly different between the two groups.
6. Ethical Considerations
This study was approved by the institutional review board of Daegu University (1040621-201809-HR-026-02). A lactation specialist nurse explained the purpose of the study and the study procedures, and received informed consent. All participants were also told that they could withdraw from the study at any time without any disadvantages.
RESULTS
1. Homogeneity Test of Clinical Characteristics between the Two Groups
There were no significant differences in LPIs' clinical characteristics between the two groups, except the length of hospital stay and their diseases. The length of hospital stay was significantly longer in the experimental group (11.9±3.8 days) than in the control group (8.7±4.3 days), and more LPIs in the experimental group had diseases than in the control group. Supportive feeding, including gavage feeding, in the experimental group was more frequent than in the control group, although this difference was not statistically significant. On the discharge day, none of LPIs had exclusive breastfeeding, and nearly two-thirds of LPIs were discharged with mixed feeding in both groups. The postmenstrual age, defined as gestational age plus weeks elapsed from birth, on the discharge day and the fourth week after discharge was around 36 weeks and 40 weeks in both groups, respectively (Table 2).
No significant differences were found between the two groups in LPIs' birth weight, type of delivery, maternal age, and maternal diseases. The birth weight of the LPIs in the experimental group and control group were 2,156±280 g and 2,296±389 g, respectively. Most of the LPIs in the experimental group (81.0%) and control group (84.2%) were delivered by cesarean section. Most of the LPIs' mothers did not have any maternal diseases (76.2% in the experimental group and 89.5% in the control group).
2. Comparison of Feeding Methods after Hospital Discharge between the Two Groups
There were no significant differences in the breastfeeding rate between the two groups at discharge, at the first week, at the second week, and at the third week. However, at the fourth week, the breastfeeding rate in the experimental group was significantly higher than that of the control group (x2=7.17, p=.028). The breastfeeding rate in the control group remained the same (10.5%) until the fourth week, while the experimental group showed a significant increase from 14.3% at discharge to 42.9% at the fourth week. After adjusting for the length of hospital stay and diseases of the newborns, the probability of breastfeeding was significantly higher in the experimental group than in the control group at the third week (odds ratio [OR]=13.70, 95% confidence interval [CI]=1.20~156.99) and the fourth week (OR=20.64, 95% CI=1.99~214.36) (Table 3).
3. Comparison of Neonatal Morbidity and Description of Hospital Visits between the Two Groups
The neonatal morbidity rate was 17.5%, and two LPIs in the experimental group (9.5%) and five LPIs in the control group (26.3%) visited an outpatient department or an emergency room for treatment, but there was no significant betweengroup difference (x2=1.95, p=.164). Even after adjusting for the length of hospital stay and diseases of the newborns, the probability of a hospital visit was not significantly different between the two groups (OR=0.32, 95% CI=0.05~2.22) (Table 4).
The main reason that all seven LPIs visited hospitals was neonatal jaundice. Six LPIs visited within the first week after discharge. One LPI visited a hospital around the third week after discharge. The feeding methods of the LPIs who visited hospitals were as follows: formula feeding in three infants, mixed feeding in three infants, and breastfeeding in one infant (Table 5).
DISCUSSION
This study investigated the influence of a BCP for LPIs who were admitted to the NICU on the breastfeeding rate and neonatal morbidity. LPIs' hospital stay in the experimental group was 3 days longer than in the control group. This fact reflects the fact that the LPIs in the experimental group had more neonatal diseases (e.g., hyperbilirubinemia, respiratory problems, and sepsis) and supportive feeding (e.g., gavage feeding) than those in the control group. This result is in line with the study of Medoff Cooper et al. [4], which reported that half of LPIs experienced neonatal health risks. However, the 8- to 11-day hospital stay in this study was longer than the 5-day length of hospitalization reported by DeMauro et al. [18].
The breastfeeding rate at the fourth week after discharge was significantly higher in the experimental group than in the control group. The breastfeeding rate in the control group remained the same (10.5%) from the day of discharge to 4 weeks after discharge. In contrast, the breastfeeding rate in the experimental group increased from 14.3% on the day of discharge to 42.9% at the fourth week. After adjusting for the length of hospital stay and diseases of the newborns, in the experimental group, the probabilities of breastfeeding at the third and fourth weeks were 13.70 and 20.64 times higher, respectively, than in the control group. This result is attributed to a BCP that combined web-based breastfeeding education with one-on-one practical lactation support according to LPIs' physical maturity and capability of feeding. In other words, as the postmenstrual age of the LPIs approached 40 weeks by fourth week after discharge, the LPIs became mature enough to be breastfed exclusively; therefore, hospital-based breastfeeding support and education for LPIs extended for 1 month after discharge.
The breastfeeding rate in the experimental group was higher than that reported in the study of Lee and Jang [14], in which 106 Korean LPIs were analyzed and a breastfeeding rate of 42.5% was reported at the fourth week, but lower than that reported in the UK 2010 Infant Feeding Survey [19], according to which 75.4% of LPIs were breastfed at 6 weeks. This discrepancy indicates that Korean LPIs are less likely to be continued to be breastfed than LPIs in other nations. This result is consistent with a study on a breastfeeding support program provided for LPIs, which showed that the exclusive breastfeeding rate in the experimental group (55%; n=20) was higher than that in the control group (25%; n=20) at the fourth week [17]. In the study by Jang and Hong [17], the higher exclusive breastfeeding rate than was observed in this study reflected the conditions of the LPIs. Specifically, 50% of the LPIs in both groups in the study by Jang and Hong [17] were recruited from a nursery and had relatively fewer health issues, whereas the LPIs in this study were recruited from the NICU alone. This result also aligns with that reported by the study of Jang and Ju [20], which provided the mothers of 53 LPIs with an infant care education program focused on promoting breastfeeding and demonstrated a significantly higher breastfeeding rate (73.1%) in the experimental group (n=26) at 1 month after discharge than in the control group (40.7%; n=27). Moreover, an integrated review of 13 breastfeeding education interventions for LPIs suggested that most interventions had positive effects on establishing exclusive breastfeeding [2]. The results of the studies by Goyal et al. [15] and Rayfield et al. [19] indicated that appropriate help and support at hospitals boosted exclusive breastfeeding by 2.21 and 3.14 times, respectively.
The neonatal morbidity rate of the LPIs in this study was 17.5%. The neonatal morbidity in the experimental group and the control group was 26.3% and 9.5%, respectively, and there was no significant difference between the two groups after adjusting for the length of hospital stay and diseases of the newborns. All the LPIs with neonatal morbidity visited an outpatient department or an emergency room due to neonatal jaundice. This is consistent with the finding of Escobar et al. [21] that the most common reason for rehospitalization of LPIs was neonatal jaundice, and the finding of Kim [22] that the major reasons for LPIs' readmission were jaundice and diarrhea. There were more hospital visits in this study than reported by Tomashek et al. [5], according to whom 4.3% of LPIs were likely to be readmitted or had an observational stay of less than 24 hours in hospitals. In addition, Jang and Ju [20] stated that none of the LPIs in the group provided an infant care education program for LPIs were readmitted, whereas one of the LPIs (3.7%) in the control group was readmitted due to enteritis. Of particular note, the feeding methods of the seven LPIs who visited hospitals were formula feeding for three infants, mixed feeding for three infants, and breastfeeding for one infant. This result is different from that of many previous studies, which reported that breastfed LPIs were more likely to have neonatal jaundice than non-breastfed LPIs [5-7].
The BCP, as a community-based program, was more effective than a hospital-based breastfeeding support program [20], perhaps because the program was not merely a one-time intervention, but was repeatedly provided in the community. Breastfeeding promotion interventions are more effective when the prenatal and postnatal education at hospitals expands to the community setting [23]. In other words, the BCP successfully reinforced the breastfeeding education provided by the hospital by expanding it into the community.
Most breastfeeding promotion programs provide education and practical support in the hospital setting, but are discontinued after discharge. In contrast, this study continued the education program for 4 weeks after discharge.
The following limitations of this study are acknowledged: Firstly, the clinical characteristics of the experimental and control groups, including length of hospital stay and diseases of the newborns, were not homogeneous. Further research that ensures homogeneity in LPIs' clinical characteristics should be performed. Secondly, the same researcher provided the BCP education and investigated between-group differences, so the potential influence of the researcher being aware of the distribution of the groups on the results cannot be completely ruled out. However, the influence of the researcher was minimized, as the breastfeeding rate was observed directly. Thirdly, even though the mothers' intention to breastfeed was included as a selection criteria, mothers' psychological variables, including breastfeeding self-efficacy and confidence, and demographic characteristics were not considered as breastfeeding-related factors. Lastly, the results have limited generalizability due to the small sample size, and the study should be repeated with a larger number of participants and a longer study period. Nonetheless, the findings of this study are meaningful in that they imply that breastfeeding education could be expanded to community settings.
The positive effects of the BCP on the breastfeeding rate and neonatal morbidity among LPIs imply that breastfeeding support programs for LPIs should be continued for a certain period of time after discharge from the hospital and that tailored education should be provided based on the health status of the mother and the infant.
CONCLUSION
This study was conducted to evaluate the effects of a BCP on the breastfeeding rate and neonatal morbidity in LPIs, and found a positive effect on the breastfeeding rate and an indistinct effect on neonatal morbidity. Above all, the breastfeeding rate improved by 4 weeks after discharge in the experimental group, whereas it remained low in the control group. In addition, five LPIs in the control group and two LPIs in the experimental group visited hospitals during 4 weeks after discharge. This implies that practical breastfeeding education and support should be provided to mothers of LPIs on an ongoing basis to promote breastfeeding. Therefore, a BCP for LPIs should be utilized in hospitals and communities to a fuller extent.