Park and Choi: Transfer anxiety in parents of children transferred from pediatric intensive care units to general wards in South Korea: a hybrid concept analysis
Abstract
Purpose
This study aimed to analyze the concept of transfer anxiety in parents of children transferred from pediatric intensive care units to general wards.
Methods
The hybrid model by Schwarz-Barcott and Kim was used to analyze the characteristics of transfer anxiety in parents of children transferred from pediatric intensive care units to general wards.
Results
Transfer anxiety was defined by the following attributes: 1) stress concerning the adaptation process, 2) concern about the child’s condition worsening due to the parent’s caregiving, and 3) involuntary changes in daily life due to the treatment. Transfer anxiety has the following antecedents: 1) uncertainty; 2) a lack of knowledge about the illness, medical devices, and caregiving; and 3) a lack of social support. It resulted in 1) caregiver burden, 2) a decrease in the capacity for coping with caregiving, 3) delays in the child’s physical and psychological recovery, and 4) decreased quality of life.
Conclusion
It is necessary to develop an assessment scale that considers the attributes of transfer anxiety in parents of children transferred from pediatric intensive care units to general wards. Furthermore, an effective nursing intervention should be developed to reduce transfer anxiety.
Key words: Patient transfer; Anxiety; Concept formation; Transitional care
INTRODUCTION
Children admitted to the intensive care unit (ICU) experience several stages of transition, such as repeated symptom exacerbation and relief, transfer to a general ward (GW), and return to the community. Thus, children and their families need to re-adapt accordingly [ 1]. The most important transition stage is the child’s transfer from the ICU to the GW. In this stage, children and their families can have positive experiences such as survival, recovery from disease, and return to the community. However, changes in treatment methods from the hospitalization period in the ICU to the direct care of children in the GW can cause anxiety and be burdensome for children’s families [ 2, 3]. In the ICU, healthcare professionals are responsible for providing treatment and care to pediatric patients. However, in the GW, primary caregivers are required to provide some care for their children, thereby causing parental fear. Moreover, caregivers must adapt to an unfamiliar environment. These changes cause psychological stress that results in transfer anxiety [ 4]. In the process of being transferred from the ICU to the GW, the consequent anxiety can lead to a decrease in the ability of children and families to cope with the disease, treatment non-adherence, and extended hospitalization [ 2, 5, 6]. In addition, it could delay children’s recovery, resulting in a decreased quality of life for children and parents [ 2, 5]. Hence, it is essential for parents to participate in their children’s treatment process since family-centered treatment can lead to positive experiences concerning the hospitalization of pediatric patients and reduce parental anxiety [ 7]. The transfer from the pediatric intensive care unit (PICU) to the GW represents a stressful situation for children and their families and requires nursing interventions [ 1, 3]. During a child’s hospitalization, parents are generally the primary caregivers. Thus, transfer anxiety may increase in uncertain situations in which the parents do not understand their child’s condition [ 8]. Recent studies have shown that more than half of the parents of children admitted to the PICU still experience psychological problems 1 month after leaving the PICU [ 9]. Unlike adults, children can quickly identify their parents’ emotions, attitudes, fears, and concerns, which can exacerbate their negative psychological state, and emotional insecurity in parents can hinder childcare. Consequently, parental anxiety affects children and their families’ quality of life during the transfer process [ 10, 11]. The role of nurses is essential for children and their families to adapt to new environments and changes [ 12]. Therefore, it is necessary to identify the nature of transfer anxiety to devise effective nursing interventions [ 13]. However, few concept analyses of transfer anxiety have been conducted, and the existing studies that have been carried out among parents of children transferred from the PICU to the GW are highly insufficient. Previous studies have identified the attributes of relocation stress in adult patients transferred from the ICU to the GW [ 14] and the attributes of the post-intensive care syndrome in children [ 15] using Walker and Avant’s method [ 16]. However, studies analyzing the attributes of psychological problems in families are insufficient. In particular, the parental role in disease recovery in pediatric patients is paramount [ 13], and the existing understanding of transfer anxiety in parents is limited. Thus, it is necessary to analyze transfer anxiety experienced by the parents of pediatric patients. Moreover, a hybrid model is useful for studying key phenomena in nursing and analyzing concepts by integrating theory and practice [ 17, 18]. Therefore, this study conducted a concept analysis using a hybrid model to investigate the attributes of transfer anxiety experienced by the parents of pediatric patients when transferred from the PICU to the GW. It aimed to analyze the concept of transfer anxiety using the hybrid model developed by Schwartz-Barcott and Kim [ 17] to collect primary theoretical data for nursing interventions targeting the parents of pediatric patients. The specific research objectives were as follows: 1) the theoretical phase was performed to tentatively define the attributes of transfer anxiety through a literature review; 2) the fieldwork phase was performed to reconfirm the results of the theoretical phase through empirical observations; and 3) the final analysis phase was performed to further identify the attributes of transfer anxiety by integrating the findings of the theoretical and fieldwork phases.
METHODS
Ethics statement: This study was approved by the institutional review board of Severance Hospital (No. 2021-1857-002). Informed consent was obtained from the participants.
1. Study Design
This was a conceptual analysis study. The hybrid model is generally useful for analyzing specific concepts meaningful in nursing based on perceptions formed in the actual clinical field through an extensive literature review and qualitative analysis of actual cases [ 19]. Therefore, in this study, the hybrid model method was judged to be more appropriate than other analysis methods for identifying the conceptual attributes of transfer anxiety felt by parents in a specific situation, such as during their child’s transfer from the PICU to the GW. Moreover, this method was thought to be helpful for identifying the characteristics specific to pediatric patients and South Korean culture.
2. Theoretical Phase
1) Data collection
In the theoretical phase, a literature review of texts about transfer anxiety was performed. The scope of the investigation was determined based on dictionary definitions of transfer anxiety, examples of anxiety in other academic fields of nursing, and transfer anxiety specific to the parents of pediatric patients. The literature review was conducted from April 15 to May 31, 2021, by combining search terms with no limitations on the year of publication. The search focused on studies examining transfer anxiety published in Korean and English. The RISS, KISS, DBpia, PubMed, and CINAHL databases were searched. Due to the small number of studies on transfer anxiety in parents of pediatric patients, the scope of the literature review was expanded from parents to families. Few studies were found that used the term “transfer anxiety”, so the keywords “transfer anxiety”, “ICU”, “family”, and “parent” were combined and searched. In the theoretical phase, the inclusion criteria were non-experimental studies, experimental studies, or literature review studies that explored anxiety in family members or parents of pediatric patients.
2) Data analysis
The searched studies were reviewed and organized using EndNote X9. A total of 91 studies were identified in the initial search, with 39 in Korean and 52 in English. Among them, 28 duplicate studies and 10 studies for which full texts could not be found were excluded. Subsequently, 33 studies were extracted after excluding 30 studies that were unrelated to this study’s aim after reviewing the titles and abstracts. After reviewing the full text, studies were selected if they included a situation that involved transfer from the ICU to the GW. Three studies in Korean and seven in English were selected for this study ( Figure 1). The literature analysis investigated the meaningful attributes of transfer anxiety by reviewing similar and related concepts concerning parents of children who transferred from the PICU to the GW. The purpose of the literature review was to compare the similarities and differences between perspectives on transfer anxiety in the academic field. However, of the 10 studies reviewed, no studies from other academic fields, such as medicine and psychology, were included.
3. Fieldwork Phase
The fieldwork phase of the hybrid model involved a process of collecting qualitative data through empirical observation for in-depth concept analysis. In addition, the researchers continued the literature review to compare data collected in the field [ 17]. Therefore, in this phase, empirical data were collected through interviews.
1) Setting and sample
This study purposively sampled inpatients at a children’s hospital in Seoul during the fieldwork phase. Schwartz-Barcott and Kim [ 17] suggested that, within the hybrid model, a manageable number of study participants who could be repeatedly contacted should be included. Therefore, participant recruitment stopped when the collected information reached saturation. This study was conducted with four parents of children hospitalized in the pediatric ward of a children’s hospital in Seoul. The inclusion criterion was parents of children hospitalized in the GW after discharge from the PICU. The exclusion criteria were parents who received psychiatric treatment, were not primary caregivers, or were unable to communicate in Korean.
2) Data collection
Data collection was conducted from April 1 to April 30, 2021. Individual interviews were conducted with four parents who agreed to participate in this study. Each interview was conducted in a private space, and the interview duration ranged from 20 minutes to 45 minutes, with an average of 30 minutes. The researcher transcribed the interview in real-time with the consent of the participants. Immediately after the interview, the transcription was moved to a Microsoft Word document and edited to remove personal identification information (name, date of birth, address, and phone number). After the fourth interview, no more new data were collected in interviews. Therefore, participant recruitment ended. To ensure the reliability of the fieldwork phase, the researcher listened to the participants’ statements objectively during the interview, and the participants’ exact words were cited in the text.
The interview questions were based on a previous study [ 20] about the adaptation to the caregiver role experienced by family members of adult patients who transferred from the ICU to the GW. The specific questions included, “How did you feel when your child was transferred from the PICU to the GW?”, “What did you expect to be difficult when taking care of your child?”, “What changed after being transferred from the PICU to the GW?”, and “How did you solve the problem?”.
3) Data analysis
After the interviews were completed for the data analysis step in this study, meaningful statements related to transfer anxiety were identified, read multiple times, and analyzed. Semantic words were determined and classified based on the transcribed data. Through this process, common, repeated statements related to transfer anxiety were grouped to derive subcategories and attributes.
4. Final Analysis Phase
The final analysis phase examined the results by combining the data collected during the theoretical analysis and empirical observation phases [ 17]. In this phase, the definition, attributes, antecedents, and consequences of transfer anxiety in parents of children who were transferred from the PICU to the GW were identified using the data from the theoretical and fieldwork phases.
5. Ethical Considerations
Ethical approval for this study was granted by the Research Ethics Committee of Severance Hospital (No. 2021-1857-002). The primary step that involved participants was the interview step of the fieldwork phase. Prior to the interviews, the researcher explained the purpose and content of the study to the participants through explanations and oral guidance. Moreover, there were no negative consequences related to the treatment process when participants did not respond to the study. Participants could also refuse participation in the study at any time during the interview, and the interview contents were not used for anything other than the study’s purpose. Written informed consent was obtained from participants who voluntarily agreed to take part in the study. The interview content did not contain personal information and was stored on computers and in locked drawers. Access was prohibited for anyone other than the researchers.
6. Rigor
The corresponding author was thoroughly familiar with the hybrid model by Schwartz-Barcott and Kim [ 17], having taught a graduate course called “Concept Development in Nursing”. She is a lifetime member of the Korean Association for Qualitative Research, has participated in qualitative research workshops, and has conducted qualitative research for years. In addition, the first author completed the “Concept Development in Nursing” course at a graduate school, was familiar with the hybrid model [ 17], is a registered member of the Academy of Qualitative Research, and has participated in qualitative research. To ensure the validity of the data analysis process in the fieldwork phase, the collected data were examined after the participant interviews after personal identification information was deleted. Moreover, the researchers read the data from interviews multiple times, extracted meaningful information related to transfer anxiety, and selected the most meaningful content related to transfer anxiety through discussion. Subsequently, common meanings were grouped and categorized using labels. To ensure credibility, the researchers routinely conducted comparison analysis and confirmation. The researchers subsequently included interviews and categories that agreed with each other in the result.
RESULTS
1. Theoretical Phase
1) Definition of transfer anxiety in parents of children transferred from the PICU to the general ward
The dictionary definition of anxiety is “the state of feeling nervous or worried that something bad is going to happen”. It is a mental health problem that causes the individual to worry so excessively that it has a highly negative effect on their daily life [ 21]. In nursing, anxiety involves an emotional response to sources that are often non-specific or unknown to the individual and refers to feelings of apprehension caused by the anticipation of danger, catastrophe, or misfortune [ 22, 23]. Therefore, transfer anxiety from the ICU to the GW can be considered a form of state anxiety, referring to the anxiety felt on a moment-to-moment basis rather than relatively stable underlying anxiety [ 24]. In other academic fields, anxiety and other words have been used to describe various forms of state anxiety related to specific situations. For example, retirement anxiety [ 25] has been used in sociology, competition status anxiety [ 26] has been used in the arts and physical sciences, and speaking anxiety [ 27] has been used in the humanities. However, there were only a few instances of the use of the term “transfer anxiety” in academic fields outside of nursing. The dictionary definition of transfer is “to move from one place to another”, “to move something/somebody from one place to another”, “to move from one job, school, situation, etc. to another”, or “to arrange for somebody to move”[ 28]. A similar term to “transfer” is “relocation”, and other studies have examined the psychological problems of adult patients moving from the ICU to the GW as a form of “relocation stress” [ 14]. The dictionary definition of “relocation” is “the act of moving, or of moving somebody/something, to a new place to work or operate” [ 29]. Thus, according to dictionary definitions, “relocation” refers to the transition to a new place, whereas transfer refers to the transition to a situation. In addition, the word “transfer” is often used in practice, including the terms “transfer out” and “transfer in”. “Transfer anxiety” can be defined as the anxiety experienced during the transfer to the GW. Consequently, in the theoretical phase, “transfer anxiety” was defined as “potential sources of stress for patients and their families that could negatively affect coping during difficult processes of disease and hospitalization” or “psychological and physical problems experienced by patients and families in transferring from the ICU to the GW” [ 2, 23, 24].
2) Measurement of transfer anxiety
According to the literature review, Spielberger’s [ 30] State-Trait Anxiety Inventory (STAI) was used to measure transfer anxiety during the transfer from the ICU to the GW. For Korean studies, the STAI was translated into Korean [ 31]. The STAI is a self-reported questionnaire to evaluate how respondents feel during a particular moment, and a higher score indicates a higher state anxiety level. However, the STAI is not suited to measuring transfer anxiety. Since state anxiety refers to one’s degree of anxiety at a particular moment, it does not account for a series of processes in which a child’s health state worsens or improves, for instance, when the child enters the PICU, when the child cannot be visited in the PICU, and when parents resume caring for the child after transfer to the GW.
3) The attributes, antecedents, and consequences in the theoretical phase
When children were transferred from the PICU to the GW, their parents had to adapt to the child’s changed appearance even if they were not psychologically prepared. Moreover, they had to face several unfamiliar situations, such as the hospital environment, caring for the child, and suspended activities of daily life [ 4, 6, 8, 24]. In addition, they had to provide direct care to their child, and they often felt worried and burdened when the monitor alarm went off or the child’s condition changed [ 4, 5, 11]. When children left the PICU, they were likely to be re-admitted due to changes in their condition. Since the experience of admitting them to the PICU remained a psychological trauma for children and their parents, parents felt anxious that their child might be admitted to the PICU again [ 5, 8, 23]. Children admitted to the PICU often faced sudden and unexpected situations, causing them and their parents to experience constant changes in their daily lives. In addition, substantial efforts and support from health care providers were required for children and parents to return to their daily lives post-discharge [ 5, 32] ( Table 1). Several studies have reported significant correlations between transfer anxiety and uncertainty. In other words, uncertain situations about diseases increased transfer anxiety [ 6, 11, 23, 32]. Moreover, transfer anxiety increased with reduced social support, such as material support, emotional support, and informational support from health care providers [ 32]. Nursing interventions based on information provision effectively reduced transfer anxiety [ 8, 33, 34]. In addition, higher transfer anxiety corresponded to a higher burden on the care provider and lower functioning against the disease and coping among family members. Transfer anxiety consequently delayed the recovery of pediatric patients and decreased the quality of life for them and their families [ 4, 11, 23, 33] ( Table 1).
4) Conceptual attributes and tentative definitions in the theoretical phase
Through the literature review, the attributes of transfer anxiety in parents of children transferred from the PICU to the GW could be defined as personal and situational factors. Personal factors included “stress concerning unfamiliar situations” and “concerns about caregiving”. Situational factors included “the possibility of the child’s condition worsening” and “changes in daily life because of treatment”( Table 1). This study tentatively defined transfer anxiety in parents of children transferred from the PICU to the GW as “an uncomfortable psychological problem experienced in parents of children transferred from the PICU to the GW”.
2. Fieldwork Phase
1) General characteristics of participants
A total of 4 parents participated in the fieldwork phase, of which one was a father and three were mothers, and their average age was 43 years old. Their children included three boys and one girl, and the average age of the children was 11 years old. Since one of the children was 22 years old, she was classified as an adult. However, she had been diagnosed with a pediatric neurological condition at a children’s hospital at the age of 6, and her physical and cognitive functions were at a preschool level. Therefore, these characteristics were considered sufficient to identify the attributes of transfer anxiety in parents of children transferred from the PICU to the GW.
The hospitalization period in the PICU ranged from 4 days to 68 days, with an average of 32.25 days. The average number of admissions to the ICU was 2 times, with a range of 1 to 3 times. All four children were diagnosed with neurological diseases, and the time of diagnosis ranged from birth to 6 years old. In addition, the reasons for admission to the ICU were acute respiratory failure for two patients and status-epilepticus for two patients ( Table 2).
2) Empirical observation in the fieldwork phase
(1) Concern about the child’s condition worsening
Concern about the child’s condition worsening referred to worries and negative feelings about the child’s health condition deteriorating due to the parent’s caregiving and requiring re-admission to the ICU ( Table 3).
I was so grateful that my child endured well in the ICU and came down to the GW quickly. However, I was so worried and anxious that my child would get worse again because of me, at first.(Participant B) The ICU nurse said I have to do suction often for my daughter and change her position often after transfer to the GW… I was worried that my daughter might go back to the ICU through my mistake. The doctor said that if she is re-admitted to the ICU after transfer to the GW, she might not be able to get transferred to the GW again. (Participant C)
(2) Lack of information on the illness
Lack of information on the illness denoted the absence of information on the child’s illness, treatment, and medical devices. In addition, it included parents’ inexperience related to the operation of medical devices ( Table 3).
This small leg has a central vein, and there was too much fluid in it, so it was hard to hug my child when he cried. If I held the wrong posture, the device (infusion pump) would ring, and that sound felt too loud to me.(Participant A) I was scared because it was my first time spending 24 hours a day with him, just the two of us. Even if I have a twin younger child at home, it is different to care for a child with a disease. Actually, no one taught me properly, so I observed what the nurses did and copied them. Even that is difficult to learn because each nurse has a different way of doing it.(Participant D)
(3) Re-adaptation to the child’s condition
Re-adaptation to the child’s condition related to the process in which parents faced their child’s condition, adapted to treatment devices, and took on the role of the caregiver after it had changed following admission to the ICU ( Table 3).
My son used to eat well by mouth, but even after he came out of the ICU, the doctor said that he should not eat using his mouth. Thus, I had to use a tube inside his nose (Levin tube), but it was the hardest for me to feed with his tube. At first, when a can (enteral nutrition formula) came during mealtime, my heart was beating very fast. Moreover, I often thought, ‘Why do you make me do this?’ However, after thinking that I was his mother and I should feed him, I ended up doing well. After that, I was not scared.(Participant B) It was still hard for me to suction and feed because I had to feed after the nebulizer and suction, make my son sit down, and not perform suction for an hour after feeding. I even had to give my son medicine on time ... There were so many things to know. I was worried that I would make a mistake even though I took notes and kept reading them.(Participant D)
(4) Involuntary changes in daily life
Involuntary changes in daily life referred to concerns about changes in the daily lives of children and their families due to the changes in their disease condition when they returned home after the completion of treatment at the hospital ( Table 3).
I was apprehensive when my son was admitted to the ICU. On the other hand, it was good that I could spend time alone and did not have big arguments with my husband. Since I was with my child again in the GW, I thought I would not have time for the rest of my daily activities. My husband does not know how to care for the child, so I have to care for him from A to Z. Even if I was doing suction for my son, my husband would tell me to stop because it was hard for him to see that. That is why we argue.(Participant A) When the ICU doctor told me that there was no other way than tracheostomy, I agreed because I could not see my child’s condition in person. However, when she came out, she had a home-ventilation machine. Moreover, there were many other monitors, and I had to suction every 2 hours. Thus, I asked the doctor to remove the machine before she was discharged from the hospital. However, the doctor said this machine could not be removed so quickly, and I was very embarrassed because no one had told me about it. I was thinking, ‘How can I take all of this home and put it somewhere?’ and ‘Can I do it at home?’ I was frustrated.(Participant C)
(5) Uncertainty
Uncertainty reflected not having clear knowledge about the child’s treatment process or prognosis in the GW after their transfer from the PICU ( Table 3).
On the day he was supposed to leave the ICU, he came out after a few days because his blood pressure was unstable. He is still using a vasopressor, but I do not know when it will stop, and I am worried that his blood pressure will drop again if medication is stopped.(Participant A)
(6) Decreased coping related to caregiving
Decreased coping related to caregiving referred to a decrease in responsiveness or participation in caregiving due to negative emotions such as anxiety ( Table 3).
At first, it took exactly 2 weeks to adapt to my child’s appearance. I could not do anything because I was unfamiliar with transferring out of the ICU. However, I practiced little by little with nurses, I got the hang of it, and it became easier than I thought. After that, I lost my fear and anxiety, and I was able to do it.(Participant C)
3) Reconfirming conceptual attributes and tentative definitions
The attributes of transfer anxiety derived in the theoretical phase were similar in the fieldwork phase. Therefore, the attributes derived from the theoretical and fieldwork phases were organized in the final analysis phase ( Tables 1, 3).
3. Final Analysis Phase
1) Definition of transfer anxiety in parents of children transferred from the PICU to the general ward
Transfer anxiety in parents of children transferred from the PICU to the GW was defined as an uncomfortable psychological phenomenon experienced by parents when adapting to changes in their child’s condition and their new roles as caregivers.
2) The attributes of transfer anxiety in parents of children transferred from the PICU to the general ward
In the final analysis phase, the results derived from the theoretical and fieldwork phases were comprehensively analyzed to identify the attributes, antecedents, and consequences of transfer anxiety experienced by parents of children who transferred from the PICU to the GW. The attributes of transfer anxiety in the parents included in this study could be divided into personal and situational factors. “Stress concerning the adaptation process” and “concern about the child’s condition worsening due to the parent’s caregiving” were considered personal factors. “Involuntary changes in daily life due to the treatment” was considered a situational factor. “Stress concerning unfamiliar situations” identified in the theoretical phase and “re-adaptation to the child’s condition” identified in the fieldwork phase were combined into “stress concerning the adaptation process”. In addition, “concerns about caregiving” and “the possibility of the child’s condition worsening” identified in the theoretical phase, alongside “concern about the child’s condition worsening” identified in the fieldwork phase, were combined into “concern about the child’s condition worsening due to the parent’s caregiving”. “Changes in daily life because of treatment” identified in the theoretical phase and “involuntary changes in daily life” identified in the fieldwork phase were combined into “involuntary changes in daily life due to the treatment”. In the final analysis phase, three attributes across two categories were identified ( Figure 2).
3) The antecedents and consequences of transfer anxiety in parents of children transferred from the PICU to the general ward
In the theoretical phase, “uncertainty”, “lack of knowledge”, “changes in the process of treatment”, and “lack of social support” were antecedents of transfer anxiety ( Table 1). Moreover, “uncertainty” and “lack of information about the illness” were identified in the fieldwork phase ( Table 3). “Uncertainty” was identified in both the theoretical and fieldwork phases; therefore, “uncertainty” was confirmed to be an antecedent of transfer anxiety in the final analysis phase. “Lack of knowledge” and “changes in the process of treatment” identified in the theoretical phase and “lack of information on the illness” identified in the fieldwork phase were combined into “lack of knowledge about the illness, medical devices, and caregiving”. Since “lack of information on the illness” identified in the fieldwork phase reflected “lack of social support” identified in the theoretical phase, “lack of social support” was also confirmed to be an antecedent of transfer anxiety in the final analysis phase ( Figure 2). In addition, the results of the fieldwork phase supported the consequences identified in the theoretical phase. Therefore “caregiver burden”, “decrease in the capacity for coping with caregiving”, “delays in the child’s physical and psychological recovery”, and “decreased quality of life” were consequences of transfer anxiety in the final analysis phase. Therefore, three antecedents across two categories and four consequences across two categories were identified in the final analysis phase ( Figure 2).
DISCUSSION
This study attempted to identify and classify concepts related to transfer anxiety in parents of children transferred from the PICU to the GW using a hybrid model [ 17]. Transfer anxiety is considered to be an important concept for maintaining continuity in nursing [ 12]. However, few nursing studies on transfer anxiety have been conducted on the parents of pediatric patients, with previous studies focusing on the families of adult patients [ 8, 11]. Thus, there was a clear need for a tentative definition of transfer anxiety in parents of children transferred from the PICU to the GW based on the essential process in pediatric nursing of concept development. “Stress concerning the adaptation process” refers to parents’ negative emotions related to adapting to changes caused by their children’s discharges from the ICU in terms of their children’s overall condition, the caregiver’s role, treatment devices, and the environment. A previous study of family members of adult patients who had been transferred from the ICU to the GW explained the process of adapting to the caregiver role as “becoming almost a nurse with hope and fear”[ 20]. In terms of relocation stress, adult patients considered the ICU to be a familiar and safe environment [ 14]. However, in terms of transfer anxiety, parents felt the ICU to be an uncertain space that did not allow them to monitor changes in the child’s condition. In addition, previous studies reported the result that “being a parent with a critically ill child is exhausting” when analyzing the transition experienced by parents of children transferred from the PICU to the GW. This result corresponds to the negative emotions experienced by parents in this study [ 35]. While the prior study focused on exhaustion rather than anxiety during the adaptation process, parents in previous studies [ 32, 35] and this study expressed negative emotions about uncertain situations, showing that negative emotions can be expressed in various ways. The nature of these emotions can be said to be similar. In the fieldwork stage, these emotions were found to be aggravated by uncertainty about the child’s illness and parents’ lack of knowledge. Moreover, an individualized education program was reported to reduce anxiety in caregivers during the transfer from the ICU to the GW [ 34]. Thus, a step-by-step and individualized education program tailored to the characteristics of children and parents’ educational needs is necessary [ 36]. “Concern about the child’s condition worsening due to the parent’s caregiving” was classified as a personal factor. In the PICU, treatment is performed entirely by the health care provider, and the visiting hours for parents are limited. However, in the GW, parents can observe their child’s treatment process 24 hours a day and participate in their care, including processes such as suction, feeding via a Levin tube, administering a nebulizer, and changing the position of the child under the guidance of a nurse [ 8]. Thus, the parents in this study felt worried and anxious about the deterioration of their child’s condition due to unnecessary or incorrect care. This feeling of anxiety was characterized by concerns about the deterioration of the child’s condition caused by the parent due to improper caregiving rather than the disease progression or another caregiver. This finding was consistent with a previous study [ 36] that showed that mothers often experienced unstable emotional reactions such as guilt due to the inability to fulfill a maternal role, concerns regarding the unfamiliar hospital environment, pain from treatment or the treatment of a child, and a feeling of responsibility for the family during hospitalization. Previous studies about post-ICU syndrome reported that a younger patient age corresponded to a higher degree of psychological stress among family members [ 37]. However, in this study, these attributes were not associated with the age of the pediatric patients. Our study was focused on in-depth interviews rather than participatory observation. Moreover, a previous study that dealt with post-ICU psychological distress in family members reported that higher satisfaction with care provided by a health care provider correlated with lower anxiety [ 37]. However, this finding was not observed in this study. Since the interviewer was a staff nurse in the ward where the child was hospitalized, the parents were unlikely to talk about treatment satisfaction because of the caregiver-nurse relationship [ 38]. Thus, future studies should identify the attributes of anxiety according to the parents’ characteristics. Moreover, it is recommended that interviewers with no relationship to the participants should perform participatory observations. Finally, “involuntary changes in daily life due to the treatment” refers to anxiety about involuntary changes in the present and future status of caregivers and patients due to changes in care needs, long-term hospitalization, leave of absence, and changes in the roles of family members. This was similar to the “physiological and psychosocial changes after relocation” attribute of relocation stress identified in a previous study [ 14] of adult patients transferred from the ICU to the GW. The attributes of post-intensive care syndrome included physical, cognitive, psychological, and social dysfunction in children [ 15]. This finding is similar in that changes occurred due to the progress of a child’s disease, but the attributes of transfer anxiety were related to negative feelings caused by these changes. Moreover, a lack of social support increased the family burden, stress, depression, and anxiety associated with care for pediatric patients [ 39]. This was similar to the “lack of social support” finding concerning the antecedents of transfer anxiety. Thus, nurses should assess the emotional states of parents, provide education on children’s diseases and treatments, and provide sufficient emotional support [ 34] while maintaining the necessary social resources [ 39]. Concept analysis is a crucial step in providing clarity for a concept that is not well defined. In nursing research, concept analysis is necessary when there are no tools to measure a certain concept or the available tools cannot assess the concept in relation to a given study population [ 40]. Therefore, this study can be the basis for future studies that explore related factors based on concept analysis and develop a measurement scale for transfer anxiety. Moreover, it can serve as a framework for devising nursing intervention programs for reducing transfer anxiety in parents by identifying its attributes, antecedents, and consequences. This study has some limitations. First, it included participants based on their child’s level of physical and cognitive function. The results might differ from the attributes of transfer anxiety in parents with infants and toddlers. Second, only one in four of the patients was female, and gender differences may not have been sufficiently assessed. Third, our data were saturated after four participant interviews during the fieldwork phase. Compared to the theoretical phase, few antecedents and consequences were derived from the fieldwork phase, which may have been due to the interview being conducted by a staff nurse in the ward. Fourth, generalizability was limited since only certain attributes could be derived by observing anxiety, and the participants’ baseline anxiety was not considered. Finally, since participants were recruited from a single institution, the results may not be generalizable to those at other institutions.
CONCLUSION
Since parents’ anxiety has an important effect on children’s health recovery and the quality of life of families, the characteristics examined in this study should be considered. There have been no previous studies analyzing the concept of transfer anxiety experienced by parents of children who were transferred from the PICU to the GW. Thus, it is necessary to develop an assessment scale that considers the attributes of transfer anxiety in parents of children transferred from the PICU to the GW. Furthermore, an effective nursing intervention should be developed to reduce transfer anxiety in parents of children transferred from the PICU to the GW.
REFERENCES
1. Son Y. Development and effects of the collaborative transitional care program for continuity of care in patients transferred to general wards from ICUs. Journal of Korean Clinical Nursing Research. 2009;15(3):143-155.
4. Lee HS, You MA, Lee SK, Son YJ. Factors influencing on burden of family members of intensive care patients: planned transfer to general ward after intensive care. Journal of the Korea Contents Association. 2014;14(5):211-223. https://doi.org/10.5392/JKCA.2014.14.05.211
 5. Lee HJ, Lee YM. The effects of education using a relocation information guidebook on relocation stress, anxiety, and education satisfaction in family caregivers of patients in neurosurgical intensive care units. Journal of Korean Critical Care Nursing. 2015;8(2):43-54.
7. O'Connor S, Brenner M, Coyne I. Family-centred care of children and young people in the acute hospital setting: a concept analysis. Journal of Clinical Nursing. 2019;28(17-18):3353-3367. https://doi.org/10.1111/jocn.14913
 8. Linton S, Grant C, Pellegrini J. Supporting families through discharge from PICU to the ward: the development and evaluation of a discharge information brochure for families. Intensive and Critical Care Nursing. 2008;24(6):329-237. https://doi.org/10.1016/j.iccn.2008.06.002
9. Yeo L. Post intensive care syndrome in parents of critically ill pediatric patients [dissertation]. Seoul: Seoul National University; 2020. p. 1-68.
10. Jeong KS, Park JO. The effects of the pre-operation provision of information on the anxiety and uncertainty of mothers with a preschool child of tonsillectomy and their satisfaction with post-operation nursing. Journal of the Korea Contents Association. 2016;16(1):158-166. https://doi.org/10.5392/JKCA.2016.16.01.158
11. Song MK, Bang KS. Uncertainty and transfer anxiety of pediatric patients' mothers upon discharge from the pediatric intensive care unit. Korean Parent Child Health Journal. 2012;15(2):80-88.
12. Cho SH, Jung JH, Won SY, Yi YH. Development of the transitional care program and its effect on patients discharged from the intensive care units. Journal of the Korean Data Analysis Society. 2016;18(5):2741-2756. 13. Lee J, Yoon JY. Concept analysis of parents' treatment adherence for an epileptic child or adolescent. Journal of Korean Academy of Community Health Nursing. 2021;32(2):205-219. https://doi.org/10.12799/jkachn.2021.32.2.205
 14. Son YJ, Hong SK, Jun EY. Concept analysis of relocation stress - focusing on patients transferred from intensive care unit to general ward. Journal of Korean Academy of Nursing. 2008;38(3):353-362. https://doi.org/10.4040/jkan.2008.38.3.353
16. Waker LO, Avant KC. Strategies for theory construction in nursing. 5th ed. Upper Saddle River, NJ: Pearson; 2013. p. 163-179.
17. Schwartz-Barcott D, Kim HS. An expansion and elaboration of the hybrid model of concept development. In: Rodgers BL, Knafl KA, editors. Concept development in nursing: foundations, techniques, and applications. 2nd ed. Philadelphia, PA: Saunders; 2000. p. 129-159.
18. Rodgers BL, Knafl KA. Concept development in nursing: foundations, techniques, and applications. 2nd ed. Seoul: Hakjisamedical; 2020. p. 133-135.
20. Kwon HK, Song M. Role adaptation processes of family caregivers with patients transferred from intensive care unit to general ward: becoming almost a nurse with hope and fear. Korean Journal of Adult Nursing. 2014;26(6):603-613. https://doi.org/10.7475/kjan.2014.26.6.603
22. North American Nursing Diagnosis Association (NANDA) International. Nursing diagnoses: definitions and classification, 2021-2023. 12th ed. Philadelphia: Thieme Medical Publishers; 2021. p 405.
23. Brooke J, Hasan N, Slark J, Sharma P. Efficacy of information interventions in reducing transfer anxiety from a critical care setting to a general ward: a systematic review and meta-analysis. Journal of Critical Care. 2012;27(4):425.e9-425.e15. https://doi.org/10.1016/j.jcrc.2012.01.009
24. Chaboyer W, Thalib L, Alcorn K, Foster M. The effect of an ICU liaison nurse on patients and family's anxiety prior to transfer to the ward: an intervention study. Intensive and Critical Care Nursing. 2007;23(6):362-369. https://doi.org/10.1016/j.iccn.2007.04.005
25. Hwang Y, Yang S. A study of the relationship between grit and mental well-being in middle-aged workers: the mediating effect of meaning in life and retirement anxiety. Korean Journal of Human Development. 2020;27(1):163-184. https://doi.org/10.15284/kjhd.2020.27.1.163
26. Kim HT. The relationship between overtraining perception, competitive state anxiety, and burnout among elite judo athletes. Korean Journal of Sport. 2021;19(3):619-629. 27. Han KY, Choi S. A study on validation of inspection tool for high school students' speaking anxiety using rasch rating model. Journal of CheongRam Korean Language Education. 2019;(70):43-73.
30. Spielberger CD, Gorsuch RL, Lushene RE. Manual for the statetrait anxiety inventory (self-evaluation questionnaire). Palo Alto, CA: Consulting Psychologists Press; 1970. p. 20-21.
31. Kim J, Shin D. A study based on the standardization of the STAI for Korea. New Medical Journal. 1978;21(11):69-75.
32. Mitchell ML, Courtney M. Reducing family members' anxiety and uncertainty in illness around transfer from intensive care: an intervention study. Intensive and Critical Care Nursing. 2004;20(4):223-231. https://doi.org/10.1016/j.iccn.2004.05.008
34. Tel H, Tel H. The effect of individualized education on the transfer anxiety of patients with myocardial infarction and their families. Heart and Lung. 2006;35(2):101-107. https://doi.org/10.1016/j.hrtlng.2005.09.001
35. Berube KM, Fothergill-Bourbonnais F, Thomas M, Moreau D. Parents' experience of the transition with their child from a pediatric intensive care unit (PICU) to the hospital ward: searching for comfort across transitions. Journal of Pediatric Nursing. 2014;29(6):586-595. https://doi.org/10.1016/j.pedn.2014.06.001
36. Bae JJ, Lee YE. Effect of nursing education program for mothers of hospitalized children on state anxiety and belief on parental role of mothers. Journal of the Korean Society of Maternal and Child Health. 2001;5(1):71-82.
38. Lee JP. Theoretical justification for the representativeness of participant (Sample)s' selection in qualitative research: focusing on mead's self-theory. Journal of Qualitative Inquiry. 2021;7(1):1-34. 39. Carlson JM, Miller PA. Family burden, child disability, and the adjustment of mothers caring for children with epilepsy: role of social support and coping. Epilepsy and Behavior. 2017;68:168-173. https://doi.org/10.1016/j.yebeh.2017.01.013
Figure 1.
Flow diagram of the literature search. ICU, intensive care unit. 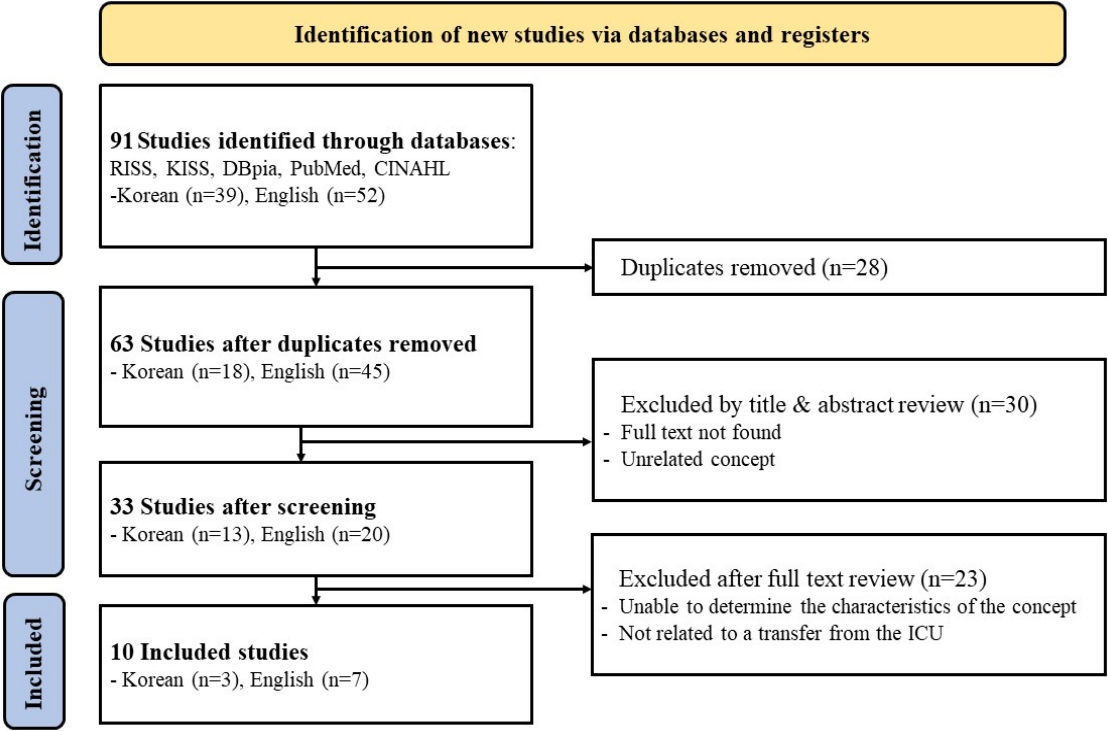
Figure 2.
Attributes, antecedents, and consequences of transfer anxiety in the final analysis phase. 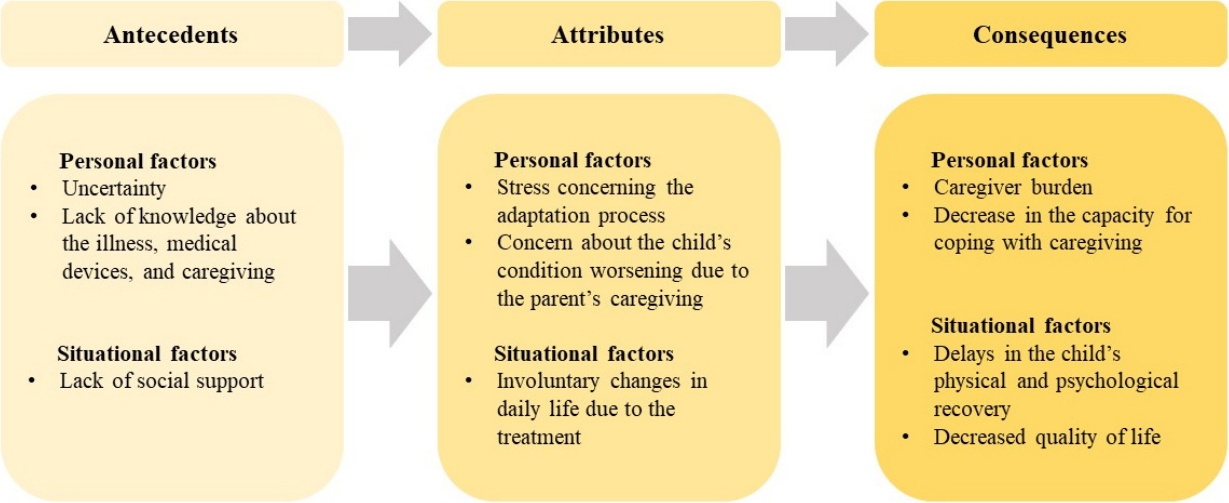
Table 1.
Attributes, Antecedents, and Consequences of Transfer Anxiety in the Theoretical Phase
|
Categories |
Personal factors [Ref.] |
Situational factors [Ref.] |
|
Attributes |
Stress concerning unfamiliar situations [4,6,24] |
Possibility of the child's condition worsening [5,23] |
|
Concerns about caregiving [5,11] |
Changes in daily life because of treatment [5,32] |
|
Antecedents |
Uncertainty [6,8,11,32] |
Changes in the process of treatment [4,5] |
|
Lack of knowledge [8,33,34] |
Lack of social support [32] |
|
Consequences |
Caregiver burden [4,23] |
Delayed recovery of the child [6,33] |
|
Decreased coping [6] |
Decreased quality of life [11] |
Table 2.
Participants' Characteristics (N=4)
|
Participant |
Relationship |
Parent's age (year) |
Child's gender/Age |
Number of admissions to the PICU |
Hospitalization period in the PICU (day) |
Child's diagnosis |
Child's age at the time of diagnosis |
|
A |
Mother |
33 |
Male/2Y 8M |
1 |
4 |
Acute respiratory failure; early infantile epileptic encephalopathy |
3M |
|
B |
Mother |
52 |
Male/18Y |
3 |
8 |
Status epilepticus; mitochondrial myopathy |
1Y 6M |
|
C |
Mother |
45 |
Female/22Y |
2 |
68 |
Status epilepticus; cerebral palsy |
6Y |
|
D |
Father |
42 |
Male/9M |
2 |
49 |
Acute respiratory failure; hypoxic-ischemic encephalopathy |
At birth |
Table 3.
Attributes, Antecedents, and Consequences of Transfer Anxiety in the Fieldwork Phase
|
Categories |
Personal factors |
Situational factors |
|
Attributes |
Concern about the child's condition worsening |
Involuntary changes in daily life |
|
Re-adaptation to the child's condition |
|
|
Antecedents |
Uncertainty |
Lack of information on the illness |
|
Consequences |
Decreased coping related to caregiving |
N/A |
|
|












