INTRODUCTION
Kangaroo mother care (KMC) refers to early, prolonged, and ongoing skin-to-skin contact between mothers and low birthweight (LBW) and/or preterm infants to overcome incubator limitations and maintain a stable temperature. KMC can be performed as early as possible and on a regular basis. It can begin at the hospital when the infant's condition is stable and continue at home after the infant is discharged. Important factors for the implementation of KMC include KMC position, exclusive breastfeeding, and the prevention and management of infection and respiratory problems [1]. KMC can be performed intermittently for at least 1 hour per session or continuously for 24 hours [1]. Previous studies [2,3] have shown that KMC can reduce the risk of death among neonates and infants. KMC also promotes exclusive breastfeeding, reduces the risk of infection, prevents hypothermia, and contributes to the growth and neurological development of infants [2-4].
Data on the number of LBW and preterm infants who undergo KMC are quite limited since most previous studies have utilized experimental designs and focused on the effects of KMC [2]. In 2018, a global assessment of 25 low-income and middle-income countries in Africa, Asia, and the Middle East found that 32% of the examined countries listed KMC as an indicator of their health service coverage [5]. However, KMC was only received by 9% of eligible infants, or 3,724 out of 41,333 infants [5].
KMC was introduced in Indonesia in the 1990s, and several KMC training sessions for health workers were conducted at the time to support its use in health service facilities, particularly in hospitals. In 2010, a study of 10 hospitals in Indonesia found that KMC had been implemented in nine of them, and four of those hospitals ultimately adopted the routine and integrated the use of KMC [6]. However, in Indonesia, KMC has not been implemented nationwide. Rather, it has mostly been implemented in teaching hospitals (medical centers that provide medical education and training for health professionals, typically affiliated with a medical school) and referral hospitals in major cities. In addition, no routine data on KMC have been reported to the Ministry of Health from those hospitals, and no national-level KMC data are currently available. Hence, the characteristics of infants who receive KMC in Indonesia have not been investigated and documented in-depth. The present study is expected to provide data and information on the characteristics of preterm and LBW infants for whom KMC could be safely provided.
KMC is an important tool for providing care to LBW and/or preterm babies, especially in areas with high rates of LBW and/or preterm infants. The prevalence rate of LBW in the Special Capital Region of Jakarta is 7.3%, with the highest rate being found in the administrative city of North Jakarta [7].
This study aimed to determine the prevalence of KMC for infants weighing less than or equal to 2,200 g at birth and to identify associations between the characteristics of infants and KMC use at Koja District Hospital. The findings of this study are expected to provide evidence for the need to increase the rate of KMC for eligible infants and strengthen KMC use at the hospital level in major cities in Indonesia and other countries in the region.
METHODS
Ethics statement: This study was approved by the ethics committee of the Faculty of Public Health, Universitas Indonesia (No. 230/H2.F10/PPM.00.02/2015). Registers and electronic medical records were used after approval from the Institutional Review Board, Koja District Hospital, and the Provincial Health Office.
1. Study Design
This retrospective cohort study was conducted to determine the prevalence of KMC and to identify associations between the characteristics of infants and KMC at Koja District Hospital in Indonesia.
2. Participants and Setting
The subjects in this study were infants who were born at or referred to and treated at Koja District Hospital during the period ranging from April 23, 2017, to January 31, 2018. Those admitted to the perinatal ward or NICU ward were eligible for this study; however, only infants who weighed 2,200 g or less were included. Infants with birthweights less than or equal to 2,200 g were considered eligible for KMC and also were the infants who were most likely to benefit from KMC. This was based on the consensus of an expert panel meeting (experts from hospitals and an association for pediatricians) that was conducted as part of a KMC research project by the Faculty of Public Health, Universitas Indonesia (FPH-UI).
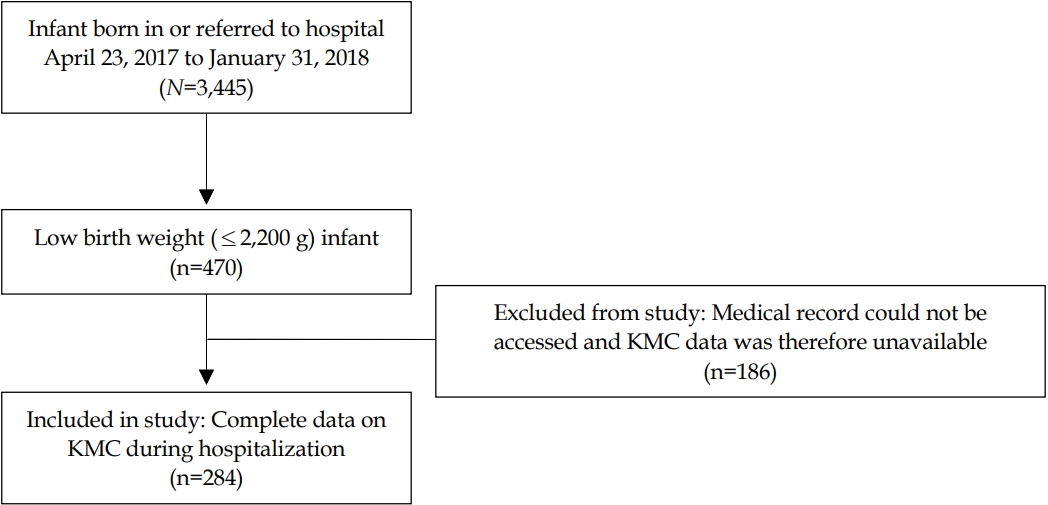
A total of 3,445 infants were hospitalized during the study period (born at or referred to the hospital). Of those, 676 were LBW infants (<2,500 g). A total of 470 infants had a birthweight that was less than or equal to 2,200 g. Of the 470 infants with birthweights less than or equal to 2,200 g, only 284 had accessible medical records that indicated whether they received KMC and could thus be used in the analysis (Figure 1).
Koja District Hospital is a referral hospital owned by the North Jakarta city government. The number of deliveries in this hospital can reach up to 300 to 400 births per month, and the total number of infant patients per year is estimated to be 4,500. The perinatal ward and neonatal intensive care unit (NICU) had a capacity of 40 and 16 beds, respectively. Koja District Hospital is one of the hospital locations where KMC research was conducted by the FPH-UI, which was funded by the USAID Partnership for Enhanced Engagement in Research (PEER) Project (2015-2019). A part of FPH-UI research project data were analyzed in this study. The research project included intervention and data collection. The intervention consisted of a refresher training on KMC and breastfeeding and assistance for all health workers at Koja District Hospital (nurses, midwives, general practitioners, obstetricians, and pediatricians) who provided services to mothers and infants, including antenatal care (ANC) services. The data were collected from infant registers in different wards, and infant medical records from hospitals were used to identify the characteristics of LBW infants and their KMC status. In addition, a survey targeting health workers and infants' mothers was also conducted. Health workers were surveyed to measure their knowledge, attitudes towards KMC, and experience/behaviors helping mothers perform KMC. Interviews with infants' mothers were also conducted to measure their knowledge, attitudes, and practices related to KMC, breastfeeding, and LBW infant care. Information on facilities (facilities, infrastructure) and procedures (standard operational procedure [SOP]) for LBW services in hospitals was also collected.
3. Study Procedure
Data were collected from infant registers and medical records at the hospital. The registers included information about infants from the delivery room, operating room, emergency room, pediatric clinic, perinatal ward, and NICU ward. Data on infants born at Koja District Hospital, either spontaneously or via a cesarean section, were recorded in the delivery room and operating room registers, while data on infants who were referred to the hospital were recorded in the emergency room and pediatric clinic registers. These registers were then synchronized with data from the registers in the perinatal ward or NICU, where infants received further care while in the hospital.
Data recorded in the registers included gestational age, birthweight, type of birth, place of birth, sex, 5-minute Apgar score, infant's transfer status to another room, maternal age, and parity. Data on infants' complications at the time of initial admission to the perinatal ward were also collected. Complications of interest to this study were those that occurred before KMC was provided, since the start of KMC, which generally takes place in the perinatal ward or NICU, is based on the presence or absence of a contraindication for KMC as defined by clinicians. Data on the use of KMC were not available in the register; therefore, these data were taken from infant medical records, which were also collected in the KMC study conducted by FPH-UI. KMC data collected from medical records included whether KMC was performed, the duration of KMC per day, the infant's age when KMC was first performed, and who performed KMC. However, since this study focused on infants who received KMC, the analysis only examined whether KMC was performed and the duration of KMC. Infants whose medical records could not be accessed during data collection were excluded from the analysis since KMC data would not be available.
4. Statistical Analysis
Univariate, bivariate, and multivariate analyses were conducted using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Univariate analysis was conducted to examine the implementation of KMC and the characteristics of infants. Categorical variables were analyzed and presented as proportions. Continuous variables were summarized and presented as means and standard deviations (SD). Differences in the proportions of categorical data were determined using the x2 test to examine relationships related to KMC use. Comparison of continuous variables associated with KMC use was performed using the t-test or the Mann-Whitney U test if the distribution of data was not normal to evaluate the statistical significance of differences in mean values for ggestational age (week), birth weight (gram), Apgar score (score), maternal age (year), and parity (number). Due to the regularity with which KMC is practiced for preterm/LBW infants (>10%), Cox regression (assigning a constant time) was preferred to logistic regression to obtain an estimated risk ratio (RR) closer to the true values, thus preventing overestimation [8]. Cox regression analysis was conducted to determine the crude and adjusted associations (RR and 95% confidence interval [CI]) between the characteristics of infants and the use of KMC. Only characteristics with a significance level of p<.250 in the crude analysis were included in the multivariate analysis.
RESULTS
Table 1 compares data on infants that were included in the analysis to data on infants that were excluded from the analysis due to having inaccessible medical records in order to identify any selection bias that might have been present. The comparison shows that there were differences in the following characteristics between infants who were included and infants who were excluded from the analysis: gestational age, type of delivery, sex, 5-minute Apgar score, and total complications prior to KMC. A higher proportion of the infants included in the analysis was preterm (mainly 34-36 weeks of gestation), had an Apgar score at 5 minutes of at least 7, and had one complication than those who were excluded. Exclusion from this study was based on the availability of KMC data; however, some data were missing for infants whose KMC data were available. Table 1 shows that the characteristics of infants who were included were generally not different from those of infants who were excluded based on the available data (type of delivery, sex, Apgar score) except with regard to gestational age.
Overall, 164 (57.7%) infants received KMC (Table 2). A majority of infants who received KMC had gestational ages of 34 to 36 weeks (73.4%) and birthweights that ranged from 1,751 g to 2,000 g (82.8%). The infants who received KMC had a mean gestational age of 34.4 weeks and a mean birthweight of 1,894 g. The infants who did not receive KMC had a mean gestational age of 32 weeks and a mean birthweight of 1,589 g. KMC was more common with preterm infants than full-term infants. More than 73% of infants with a gestational age of 34-36 weeks and slightly more than 68% of infants with a gestational age of 32-33 weeks received KMC while they were hospitalized, compared to almost 54% of non-preterm infants. The pattern for birthweight was similar to that of gestational age. A higher proportion of infants whose birthweights ranged from 1,501 to 1,750 g received KMC than infants whose birthweights ranged from 2,001 to 2,200 g. There were 18 infants in this study weighed less than 1,000 g, none of them received KMC.
Most of the infants who received KMC were born in the hospital (60.9%), had 5-minute Apgar scores of at least 7 (65.2%), had never been admitted to the NICU (62.4%), and had one complication when admitted to the perinatal ward (61.7%). Among the 284 infants, a high proportion of stable infants who did not receive treatment in the NICU and had Apgar scores of at least 7 received KMC. However, more than half (57.4%) of infants with Apgar scores of 5 or 6 also received KMC. A majority of the infants with complications who received KMC had one complication when admitted to the perinatal ward (61.7%). There were no differences in the proportion of infants who received KMC based on the type of delivery, sex, maternal age, and parity (Table 2). KMC in this study was performed intermittently in all instances, with an average duration of 2 hours and 54 minutes per session per day (Table 3). KMC was practiced in 1 session per day in most cases in this study.
Table 4 shows the crude probability of receiving KMC according to infants' characteristics and the adjusted probability according to gestational age, birthweight, place of birth, 5-minute Apgar score, NICU treatment status, and the number of complications. Based on these characteristics, infants who weighed more than 1,500 g were 2.16 times more likely to receive KMC than infants with birthweights of 1,500 g or less (95% CI: 1.20-3.89), which was a statistically significant finding. Although it was not statistically significant, KMC tended to be performed more often for infants with gestational ages of 32 weeks or higher and who did not receive treatment in the NICU, with adjusted RRs of 1.41 (95% CI: 0.85-2.35) and 1.43 (95% CI: 0.80-2.58), respectively. There was no difference in the likelihood of KMC according to Apgar score, referral status, or the number of complications.
DISCUSSION
This study examined the use of KMC in a referral hospital for infants who weighed less than or equal to 2,200 g at birth. There has been a lack of studies on the use of KMC in hospitals according to infant characteristics in developing countries, particularly in Indonesia. Our study aimed to examine associations between infant characteristics related to KMC and the use of KMC, especially concerning preterm and LBW infants who would potentially benefit from KMC the most. The findings of this study are expected to provide evidence that can be used to strengthen the use of KMC at the hospital level in major cities in Indonesia and other similar countries.
The proportion of infants who received KMC in this study was 57.7% (n=164). Using a worst-case scenario in which it was assumed that none of the excluded infants received KMC, it was estimated that at least 34% of the 470 included and excluded infants received KMC during hospitalization. The rate of KMC use in this study, following KMC refresher training and mentoring, was higher than that of other studies in Indonesia [9,10]. While KMC was first introduced in Indonesia in the 1990s, the full scope of its use has not been examined since most studies on KMC have been qualitative or, if they were descriptive studies, only included infants who received KMC [9,11]. The only studies to have evaluated the proportion of KMC use in Indonesia were conducted across 8 hospitals and were based on a national survey. A post-intervention assessment conducted across 8 hospitals in Indonesia in 2010, including teaching hospitals, district hospitals, and hospitals specific to mothers and children, showed that approximately 21% of the 979 LBW infants included in the sample underwent KMC [9]. Other data from the 2018 National Survey in Indonesia (Basic Health Research) [10] showed that the proportion of LBW infants who received KMC was 21.7%.
In Indonesia, KMC is part of the essential neonatal service for infants aged 6 hours to 28 days, as stated in the Regulation of the Minister of Health of the Republic of Indonesia No. 53 of 2014 [12]. The regulation states that KMC could be provided for infants who weigh less than 2,500 g and who do not have health problems/complications, breathing and drinking difficulties, seizures, or diarrhea, and if the mother is healthy and willing to perform KMC [12]. Despite this regulation, KMC is implemented inconsistently in hospitals in Indonesia in terms of eligibility criteria, duration, initiation, and other factors [9].
In Ethiopia and Zambia, KMC in hospital was practiced with 41.9% and 60% of preterm and/or LBW infants, respectively [13,14]. Furthermore, a rapid assessment of 25 low- and middle-income countries in Africa, Asia, and the Middle East found that only 9% of eligible infants received KMC [5]. Comparisons in coverage are quite difficult to generalize given that the criteria for KMC eligibility, duration, initiation, and other factors may vary across studies. For example, this study found that KMC was provided intermittently for approximately 2 to 3 hours per session per day, while a study from Zambia reported that KMC was provided for a minimum of 20 hours per day [14]. Another rapid assessment examining KMC in 25 countries reported a KMC duration of at least 18 hours per day [5]. In Indonesia, KMC is mostly practiced intermittently, regardless of duration [9,10].
1. Gestational Age
This study showed that infants with a gestational age of at least 32 weeks were more likely to receive KMC, although the finding was not statistically significant. This may be related to the superior reflexes and coordination related to swallowing and sucking of LBW infants with a gestational age of at least 32 weeks [15], considering that the Indonesian regulation on KMC includes not having drinking difficulty as a criterion for KMC [12]. In addition, significantly preterm infants are generally still very unstable and require more intensive care. Although the criteria for a stable infant to receive KMC generally can still vary and lack specific guidelines, another study classified the stability of infants according to their ability to breathe on their own without an assistive device and not requiring intravenous fluids [16]. Thus, health workers and mothers likely have medical concerns about non-stable infants receiving KMC, especially significantly preterm or unstable infants, due to possible negative consequences such as dislocation of medical devices (e.g., intravenous lines, catheters, nasogastric tubes) or the contraction of nosocomial infections in the NICU [17,18]. A study from the United States found that the average gestational age of infants who received KMC was around 33 weeks, with KMC being performed when the infant was in a stable condition [18]. However, another study that included infants in a NICU with a gestational age less than 32 weeks found that KMC could be initiated after several days once the infant was considered to be in stable condition by a neonatologist [19,20]. Infants with a gestational age less than 32 weeks generally have a longer stay in the NICU, leading to more anxiety among the infant's family members, which could lead to a longer period of more intense KMC education during the infant's hospitalization [19]. This can provide an opportunity for more successful KMC for very preterm infants.
Our study also found that the proportion of full-term infants (53.7%) who received KMC was lower than that of preterm infants (73.4% among infants with gestational ages of 34 to 36 weeks and 68.1% among infants with gestational ages of 32 to 33 weeks). KMC is intended primarily for preterm and/ or LBW infants; however, several other studies have shown that KMC can also be practiced with full-term infants [21]. A full-term LBW infant may not require a long duration of hospitalization; therefore, KMC may only be performed for a few days before the infant is discharged, and the brief experience of KMC may not provide the mother with sufficient confidence to continue KMC at home if it is needed [9,22].
2. Birthweight
The present study found that infants with a birthweight above 1,500 g were twice as likely to receive KMC than infants with a birthweight below 1,500 g. More than 50% of infants with birthweights between 1,501 and 2,200 g received KMC. The World Health Organization recommends for KMC to be practiced until the infant reaches 40 gestational weeks or weighs 2,500 g [1]. The SOP of KMC in the study hospital, which was developed in 2016, stated that KMC should be used for infants who weigh less than 2,000 g and are in stable condition, as indicated by a pulse of 120 to 160 beats per minute, a respiration rate of 30 to 60 breaths per minute, and a temperature of 36.5°C to 37.5°C for at least 3 consecutive days. Despite the SOP stating that KMC should be used for infants who weigh less than 2,000 g, this study found that 55.2% of infants with birthweights between 2,001 g and 2,200 g received KMC. However, the proportion of KMC use was lower than that of infants with birthweights between 1,751 g and 2000 g.
The results of this study also showed that 24.0% of LBW infants with birthweights between 1,001 g and 1,500 g received KMC. This rate was lower than that of another study that examined the use of KMC in Zambian teaching hospitals, where 60.8% of LBW infants who weighed 1,000 g to 1,400 g received KMC [14]. A qualitative study at the study hospital showed that health workers tended to be more confident performing KMC when the infant weighed at least 1,800 g [23]. According to information from other hospitals in Indonesia, although KMC implementation criteria are not always based on birthweight, KMC is more likely to be carried out with infants who are stable, as determined by the infant's ability to suck well, move, and cry actively and if the infant does not require treatment in an incubator [23]. In this study, no infants whose birthweights were under 1,000 g were found to have received KMC, which corresponds to the results of a study from the United States that found that nurses were not confident enough to provide KMC for infants who weighed less than 1,000 g [24].
3. Place of Birth
The distance between one's home and the hospital and daily travel to a hospital to perform KMC with a newborn infant can pose problems for mothers and families [9], particularly if the economic status of the family makes it difficult to afford daily transport to the hospital or secure accommodations near the hospital. Meanwhile, families with a relatively high socioeconomic level or that are more educated are more likely to seek to continue KMC since they are also more likely to be aware that the benefits outweigh the financial burden [22]. In this study, 50% of referred infants came from primary-level health facilities or hospital networks located more than 10 km from the study hospital. Although there is no guarantee that parents of infants born at the hospital live nearby, the distance barrier is likely worse for mothers of referred infants. Our data showed that 60.9% of infants born at the hospital received KMC as opposed to only 44.4% of referred infants, and the difference in proportion was statistically significant (x2=4.19, p=.041). However, multivariate analysis showed only a slight, non-statistically significant increase in the probability of KMC use (RR=1.16, 95% CI: 0.71-1.69, p=.547). This suggests that KMC could also be performed safely for referred infants with 1 or more complications upon admission to the hospital.
4. Neonatal Intensive Care Unit
Infants who were not treated in the NICU were almost 1.5 times more likely to receive KMC, although the result was not statistically significant. This study found that KMC was provided for 62.4% of infants who were not treated in the NICU, but only 31% of infants who were treated in the NICU. A study from China found that limited access to the NICU and a short duration of stay during visits were also factors that made KMC difficult [22]. KMC for infants in the NICU still requires more detailed guidelines and careful assessment to ensure that it can be practiced safely while also continuing to provide optimal benefits. Adequate knowledge and preparedness of trained medical personnel, such as pediatricians and nurses, as well as the awareness that KMC can be provided to vulnerable infants, are important for supporting the use of KMC in the NICU. The results of a 2002 hospital survey from the United States showed that around 67% of infants in a level 3 NICU received KMC, although more up-to-date data are required [25]. If an infant who was initially treated in the NICU improves, and the family is educated about KMC while the infant is being treated and willing to perform KMC, then KMC can be performed [19,20].
5. Complications and Apgar Scores
This study found that there was no significant difference in the likelihood of KMC according to an infant's 5-minute Apgar score and the number of complications experienced by the infant. This means that there was an equivalent likelihood of using KMC for infants with Apgar scores of 5 or above and those with Apgar scores of less than 5 (RR=1.16, 95% CI: 0.62-2.19, p=.647), and the likelihood of using KMC was also similar between infants with zero or one complication and those with more than one complication (RR=1.19, 95% CI: 0.52-2.72, p=.686). Among the 12 infants with an Apgar score of 3, five received KMC and survived. In addition, among the 14 infants with an Apgar score of 4, four received KMC and survived. Therefore, with careful assessment and follow-up by an experienced neonatologist, KMC can be provided to some infants with Apgar scores of less than 5 (3-4) and infants with more than one complication. This result is similar to the findings of previous studies that found that complications and Apgar scores were not considered when deciding to perform KMC [20,26]. In one of the aforementioned studies, KMC was initiated on the 24th day after birth for preterm infants with a gestational age of 25 to 28 weeks and an average Apgar score of 4.5 [20]. In our study, the mean age at which infants began to receive KMC was 10 days for infants with an Apgar score of 3 to 4 and 23 days for infants with more than one complication. KMC was initiated after each infant's condition stabilized.
When the infant's condition enables them to be considered eligible for KMC, there is a strong chance that KMC will be performed for infants with birthweights above 1,500 g, infants with a gestational age of 32 weeks or more, and infants without a history of NICU treatment. In addition, with careful assessment, close monitoring, and adequate follow-up, KMC can be performed safely for referred infants, infants with Apgar scores of less than 5 (3-4), and infants with more than one complication. This indicates that there was an equivalent probability of KMC being performed for infants with Apgar scores of less than 5 and those with scores of 5 or more, infants who were referred to the hospital rather than born in the hospital, and also for infants who had zero or one complication versus those with more than one complication. This finding indicates that KMC could be performed even for infants with a low Apgar score or complications with further assessment and close monitoring of the infant's condition by clinicians. Thus, our study provides evidence that KMC could be performed for high-risk newborns with Apgar scores of 3 or above or with more than one complication.
To ensure that eligible LBW infants receive the optimum benefits of KMC, in addition to the previously mentioned infant characteristics, the quality of KMC must also be high. The elements of KMC quality include the duration, position, and breastfeeding status. The duration of intermittent KMC can be increased (recommended for 18 hours or more) or adjusted to be performed continuously [27]. Continuous KMC can be performed at the hospital in this study since it has a dedicated room with 3 beds where mothers of infants can stay to perform KMC free of charge.
To improve the use of KMC for small infants, expecting parents should be educated during antenatal care visits, especially if there are indications of preterm delivery, and during and prior to labor to provide mothers with KMC knowledge [17,28]. Furthermore, longer and more intensive KMC education during hospitalization could improve the willingness of mothers to perform KMC as well as their confidence. This could minimize the likelihood of missing the window for providing KMC to eligible infants [9,19,22]. Health workers, especially nursing staff, play a vital role in promoting KMC due to their role in caring for infants, educating mothers about infant care, and performing daily monitoring of infants [29]. Hence, periodic training, meetings, workshops, and knowledge sharing within professional and hospital networks are necessary to improve KMC knowledge, acceptance, and confidence among nursing staff [30].
There are several limitations to this study due to missing data, particularly missing medical records and missing data for some variables in the available medical records. In addition, no information was collected on the characteristics of mothers and families, such as education level, occupation, socioeconomic status, and family support, which are factors that can contribute to the acceptance of KMC by the mother and family.
CONCLUSION
The results of this study showed that KMC can be provided safely to infants who weigh more than 1,500 g at birth, who have a gestational age of at least 32 weeks, and who have never been treated in the NICU. In addition, it is also relatively safe to provide KMC to high-risk infants with Apgar scores as low as 3 or 4, who are born in a different hospital, or who have more than one complication as long as the infant is closely monitored by competent clinicians. It is recommended that KMC be provided to all eligible LBW infants with a longer duration of KMC and better KMC quality, even for high-risk neonates. KMC education should be provided for mothers and family members during ANC visits and labor to promote immediate skin-to-skin contact and during hospitalization to improve the likelihood and quality of KMC. To improve KMC knowledge, acceptance, and confidence among nursing staff, training, meetings, workshops, and knowledge-sharing within professional and hospital networks should be conducted regularly.